⚠️ The X-Ray We Keep Refusing to Read
A World on the Edge: Global Pandemic Preparedness - 2026 GPMB Report
Fractures in the map—
trust, more fragile than the glass—
one flame, the world holds.
With every article and podcast episode, we provide comprehensive study materials: References, Executive Summary, Briefing Document, Quiz, Essay Questions, Glossary, Timeline, Cast, FAQ, Table of Contents, Index, Polls, 3k Image, Fact Check, Comic and
Street Art at the very bottom of the page.
Soundbite
Trailer
Essay
There is a particular kind of denial that doesn’t look like denial at all. It looks like competence. It looks like wastewater genomics and billion-euro research partnerships and centralized crisis agencies with acronyms nobody can pronounce. It looks, from a certain altitude, like progress.
And it is progress. Let’s be honest about that first, because honesty cuts both ways.
In May of 2026, epidemiologists watching the global health radar saw something unsettling: a woman in rural Cambodia, five children in China, a salmonella cluster tied to sprouted microgreens in Europe, a cruise ship quarantined in open water for a hantavirus cluster that shouldn’t have been on a cruise ship at all. Individually, these read as noise. The kind of thing you scroll past. Collectively, they form a picture that trained eyes cannot unsee—not a single clean break in the bone, but a dozen hairline fractures glowing across the x-ray of the world.
The scientists who study these things for a living call it a VUCA world. Volatile. Uncertain. Complex. Ambiguous. They are not being dramatic. They are being precise.
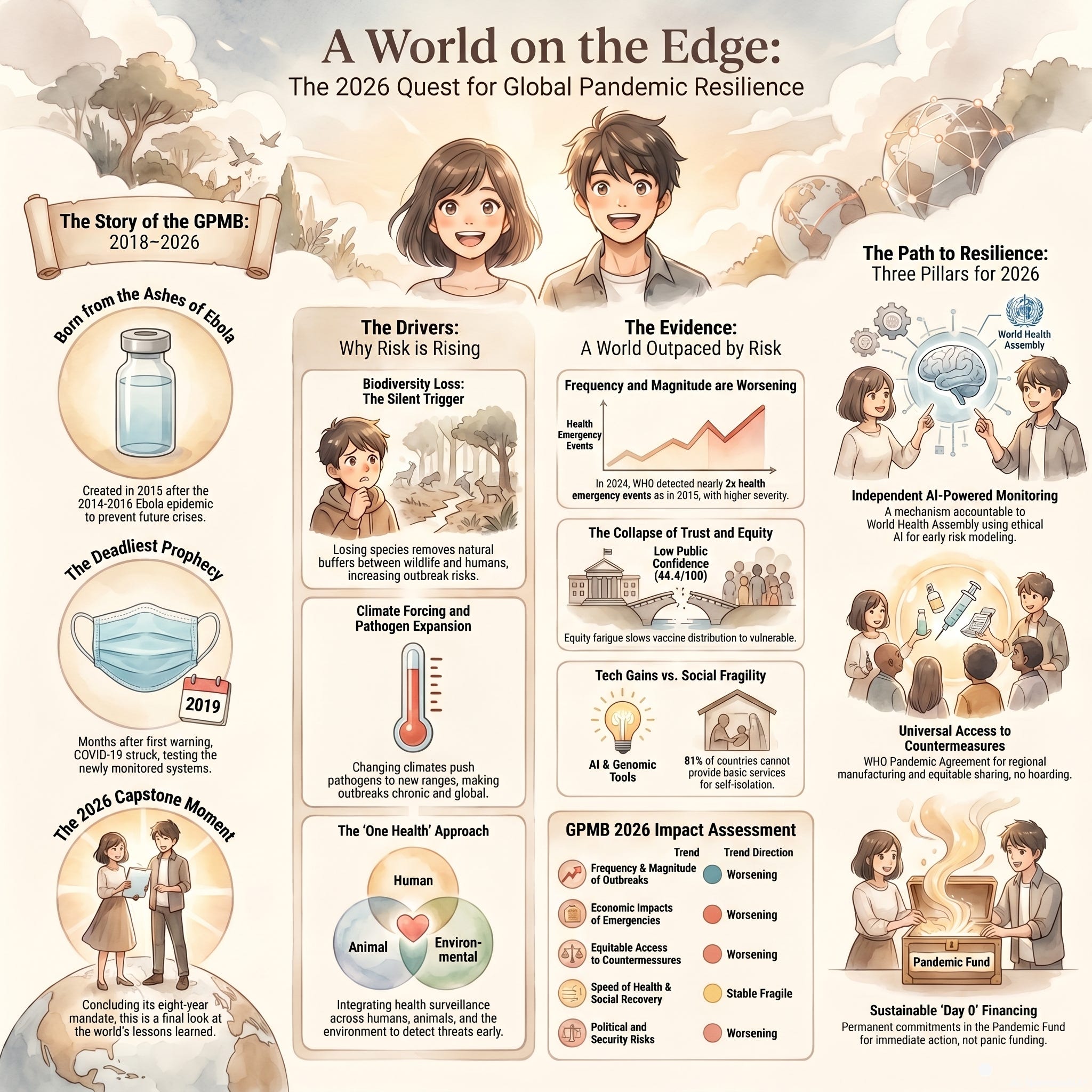
The Global Preparedness Monitoring Board—the GPMB, born from the ruins of the West African Ebola epidemic—published their 2026 capstone report with the title A World on the Edge. These are not people given to theatrical language. These are former heads of state, leading epidemiologists, and economic theorists who watched their 2019 warning go unheeded, watched COVID-19 arrive exactly as they predicted, watched millions die, and came back anyway. That they are still sounding the alarm is, paradoxically, one of the more hopeful things happening in global health right now.
Here is what they found: the trajectory of pandemic risk is moving in the wrong direction.
That sentence deserves to sit for a moment. After COVID. After mRNA vaccines developed in record time. After billions of dollars pledged to preparedness. The risk is still climbing.
How?
The biology is almost the distraction. The avian influenza strains probing human hosts in Cambodia and China are doing what viruses have always done—they are spinning the genetic roulette wheel, testing mutations, looking for the configuration that lets them travel efficiently from one human respiratory tract to another. Every zoonotic spillover is another spin. Most are dead ends. One will not be. This is the nature of evolution and it is not new information. What has changed, what the GPMB understands with a depth that doesn’t always translate into news cycles, is the world the virus will land in when that spin finally pays off.
The engine of outbreaks is us.
Biodiversity loss. Deforestation. Rapid urbanization pressing human settlements against the wild edges where viruses circulate in animal populations that have held them quietly for millennia. We have bulldozed the buffer zones. A bat that used to live fifty miles from human settlement now roosts in the rafters of a pig farm. The pig becomes a mixing vessel. The farmer becomes a case. The farmer boards a plane. This is not science fiction—it is ecology, and it has been unfolding in slow motion for a century. Climate change accelerates it, pushing disease vectors into latitudes and altitudes they have never before inhabited.
None of this would be insurmountable if our societal infrastructure were sound. But the Global Health Security Index—the global scorecard for pandemic preparedness, assessed across 195 countries—returned an average score of 38.9 out of 100. During COVID-19. During the ultimate stress test. That score, by any academic measure, is a failing grade. And it had barely moved from the 2019 baseline.
Seventy-three countries lack sufficient hospitals, clinics, and trained health workers. Sixty-five percent of countries lack a published national emergency response plan for pandemic-potential disease. And perhaps most critically: 81 percent of countries provide no wraparound economic support—no food delivery, no income replacement—to enable their citizens to actually follow quarantine instructions. You can write the most brilliant public health protocol in the world, but if a bus driver living paycheck to paycheck is told to stay home for two weeks without pay, the protocol fails. The economy becomes the engine of transmission.
And yet.
There are countries doing extraordinary things. The United States established wastewater surveillance networks across thousands of municipalities—a passive, anonymous, real-time genomic radar system that detects viral RNA in sewage before the first patient walks into an emergency room. Europe launched the BE Ready Partnership, a 1.8 billion euro coordinated research infrastructure across 81 organizations in 27 countries. Japan created a permanent central crisis management authority reporting directly to the Cabinet. China elevated its public health apparatus and applied advanced surveillance to combat tuberculosis with documented success. South Korea—and this is the one that gives genuine hope—ran pandemic simulations that included not just virologists but local mayors, religious leaders, and union heads. Because a vaccine that the public refuses to take is not a vaccine at all.
This is real. This matters. These are not press releases—they are architectural shifts in how nations think about collective security.
But the GPMB looked at all of this magnificent fortress construction and arrived at a difficult conclusion: the foundation is still collapsing.
The bedrock is trust. And trust is fractured.
Citizens distrust their governments after the chaotic, contradictory communications of previous crises. Nations distrust each other after the vaccine nationalism of 2021, when wealthy countries hoarded supplies and enacted export bans while lower-income nations watched and took careful notes about what global solidarity actually means in practice. Developing nations distrust a system that asks them to share outbreak data immediately—for the greater good—and then watches pharmaceutical companies in wealthy countries manufacture vaccines from that freely shared data, sell 90 percent of the initial supply to the countries that already have the best hospitals, and ship the remainder as charity.
Why would any rational nation pull the fire alarm quickly under those conditions?
This is where the GPMB’s most quietly radical idea lives. Day-Zero financing. The concept is elegant: when a nation identifies a novel outbreak and reports it to the WHO, an immediate, guaranteed injection of capital arrives—not a loan, not a pledging conference, not a promise—but instant funds to compensate for the inevitable economic devastation of pulling the alarm. It makes doing the right thing for global health economically survivable. It aligns the incentives, which is the only durable way to change behavior.
The GPMB is also demanding binding international agreements—not voluntary charity—that guarantee developing nations a share of any medical countermeasures developed from their shared data. The Pathogen Access and Benefit Sharing System, PABS, is their proposed framework. It replaces goodwill with obligation.
None of this is naive. None of this is asking humanity to become something it has never been. It is asking governments to design systems that work with human nature rather than against it. People share when sharing is safe. Nations cooperate when cooperation doesn’t bankrupt them. Trust builds when the system demonstrably rewards honesty.
Doris Lessing once wrote that the most dangerous thought a human being can have is the thought that things must remain as they are. Margaret Atwood reminds us, repeatedly, that the future is not something that happens to us—it is something we build, or fail to.
The x-ray of the world in May 2026 is not a death sentence. It is a diagnostic. And unlike a broken bone, the fractures it reveals are not in our biology. They are in our agreements, our economic systems, our willingness to extend the definition of “us” to include the woman in Cambodia and the child in China and the health minister in a lower-middle-income country holding a terrifying sequence result and staring at a phone they are afraid to pick up.
The technology is already miraculous. The Silicon Guardians are watching. The wastewater knows.
What remains is the older, harder work: building the kind of world where a single village’s fire alarm is everyone’s emergency. Where the globe foots the bill instantly, because everyone finally understands that containing an outbreak in one small place is a service to the entire species, and the species has decided it would like to survive.
That decision is still ours to make.


Link References
A world on the edge global pandemic preparedness
A world on the edge – Priorities for a pandemic-resilient world, 2026 GPMB report
Hantavirus cluster linked to cruise ship travel, Multi-country
Biodiversity loss is biggest driver of infectious disease outbreaks, says study - The Guardian
Does climate change increase the spread of infectious disease?
Korea runs landmark pandemic simulation exercise to strengthen outbreak readiness
2026-WCP-0024 Draft.docx - ECDC
Individual References
Ibrahim Abubakar Pro-Provost (Health) and Dean, Faculty of Population Health Sciences, UCL
Victor J. Dzau President of the United States National Academy of Medicine and Vice-Chair of the US National Research Council
Zijian Feng Professor at the School of Public Health and Emergency Management, Southern University of Science and Technology; Senior Research Fellow of the Chinese Center for Disease Control
Jayati Ghosh Professor of Economics at the University of Massachusetts Amherst
Naoko Ishii Professor and Executive Vice President at the University of Tokyo
Ilona Kickbusch Founder and Chair of the Global Health Centre at the Graduate Institute of International and Development Studies in Geneva
Matthew Stone Veterinary epidemiologist and former Deputy Director-General of the World Organisation for Animal Health (WOAH)
Jason Rohr Lead researcher and Professor at the University of Notre Dame
Esmita Charani Associate Professor at the University of Cape Town and Reader in Infectious Diseases, AMR, and Global Health at the University of Liverpool
Jon Stokes Assistant Professor in the Department of Biochemistry and Biomedical Sciences at McMaster University
Brian Hie Stanford Science Fellow at the Stanford University School of Medicine
Frank Møller Aarestrup Professor at the Technical University of Denmark and Head of Division at the National Food Institute
Thomas Van Boeckel Spatial epidemiologist at ETH Zurich
Catrin Moore Research Group Leader for the Oxford Global Burden of Disease Project at the University of Oxford
Claire Chandler Co-Director of the Antimicrobial Resistance Centre at the London School of Hygiene and Tropical Medicine
John Stelling Co-Director of the WHO Collaborating Center for Surveillance of AMR at Brigham and Women’s Hospital
David Aanensen Director of the Centre for Genomic Pathogen Surveillance at the Big Data Institute, University of Oxford
Satyajit Sarkar Research Scientist and Project Coordinator at the International Vaccine Institute (IVI) Email: satyajit.sarkar@ivi.int
Nicole Tischler President of the International Society for Hantaviruses and researcher at Fundación Ciencia & Vida, Universidad San Sebastián (USS), Chile
Piet Maes President-Elect of the International Society for Hantaviruses and researcher at Université Libre de Bruxelles (ULB), Belgium
Colleen B. Jonsson Secretary of the International Society for Hantaviruses and researcher at the University of Tennessee Health Science Center, USA
Episode Links
Apple Podcast
Youtube
Available for broadcast on PRX
PRX Series
Other Links to Heliox Podcast
YouTube
Substack
PRX ( Public Radio Exchange)
Podcast Providers
Spotify
Apple Podcasts
Patreon
FaceBook Group
STUDY MATERIALS
Global Infectious Disease Threats and National Preparedness: A 2026 Strategic Briefing
Executive Summary
As of 2026, infectious disease outbreaks have transitioned from sporadic crises to chronic features of the global security environment. This escalation is driven by systemic anthropogenic changes, including climate volatility, biodiversity loss, and increased global connectivity. Despite significant technological advancements in genomic surveillance and data modernization, the Global Health Security (GHS) Index reveals a persistent lack of readiness, with a 2021 global average score of only 38.9 out of 100. No country currently sits in the top tier of preparedness.
National strategies are evolving from reactive crisis management toward proactive, resilient frameworks. Key trends include the integration of “One Health” philosophies—recognizing the link between human, animal, and environmental health—and the development of “100-Day Missions” to compress vaccine development timelines. However, critical gaps remain in vaccine inventory management, public trust, and the protection of vulnerable populations.
--------------------------------------------------------------------------------
I. Scientific and Environmental Drivers of Pathogenic Risk
The increased frequency of outbreaks is fundamentally rooted in human-driven transformation of natural ecosystems.
1.1 Climatic Forcing
Climate change acts as a force multiplier by altering the environmental niches of pathogens and vectors.
Vector Expansion: Rising temperatures increase the metabolic and reproductive rates of ectotherms like mosquitoes, ticks, and rodents. Warmer conditions accelerate the extrinsic incubation period, allowing pathogens to develop faster within vectors.
Water-Borne Pathogens: Rising sea temperatures favor the growth of bacteria such as Vibrio cholerae and Shewanella. Extreme weather events, including floods and cyclones, compromise wastewater systems and mobilize pathogens, leading to outbreaks of typhoid and diarrheal diseases.
1.2 Biodiversity Loss and the “Dilution Effect”
Research indicates that biodiversity loss is the primary environmental driver of infectious disease outbreaks, surpassing climate change in impact.
The Dilution Effect: High-biodiversity ecosystems contain diverse species that act as “dead-end” hosts. When biodiversity declines, these hosts disappear, leaving “generalist” species (e.g., specific rodents or birds) that are highly competent reservoirs for zoonotic diseases.
Deforestation: Land-use changes increase “edge effects,” maximizing human-wildlife contact and facilitating zoonotic spillover.
1.3 Urbanization and Social Vulnerability
Connectivity: Global travel allows localized outbreaks to become pandemics within months, as pathogens traverse continents faster than their incubation periods.
Density: While urban areas often have better sanitation, high population density facilitates the rapid spread of airborne and sexually transmitted infections.
--------------------------------------------------------------------------------
II. Global Health Security Metrics (2026 Analysis)
The GHS Index benchmarks 195 countries across six categories. The 2026 data shows that theoretical capacity often fails to translate into effective response.
2.1 Top 10 National Rankings (GHS Index)

2.2 Key Findings on Global Weaknesses
Neglect of Vulnerable Populations: Only 33 countries have emergency plans that include specific considerations for vulnerable groups.
Financial Stagnation: 155 out of 195 countries have not allocated dedicated national funds for epidemic preparedness in the last three years.
Health System Fragility: 70% of countries show insufficient capacity in clinics and hospitals, including staffing shortages.
--------------------------------------------------------------------------------
III. National Strategy and Execution Models
3.1 United States: Data and Genomic Surveillance
The U.S. strategy focuses on the “Moving Forward” initiative at the CDC, prioritizing real-time threat detection.
Public Health Data Strategy (PHDS): Aims for a modernized, interoperable ecosystem using AI and machine learning to synthesize international health alerts.
Advanced Molecular Detection (AMD): Leveraging five Pathogen Genomics Centers of Excellence to enhance molecular epidemiology.
Wastewater Surveillance: Establishing a sustainable network for early detection of respiratory viruses without individual testing.
3.2 Canada: One Health and Avian Influenza
Canada leads in “One Health” integration but faces significant logistical hurdles.
H5N1 Response: Between 2021 and 2026, H5N1 affected every province, resulting in the culling of ~17.3 million commercial birds and $360 million in compensation.
Vaccine Management Issues: A 2026 audit revealed that 95% of the 870,000 doses of avian influenza vaccine secured by the Public Health Agency of Canada (PHAC) expired unused in February 2026.
Species at Risk: Surveillance has expanded to include endangered species like the Whooping Crane (population ~550), which saw positive detections in 2025.
3.3 European Union: Coordination and Research
The EU utilizes the Health Emergency Preparedness and Response Authority (HERA) for centralized management.
BE READY Partnership: A €120 million initiative launched in 2026 to bridge the gap between research, policy, and industry.
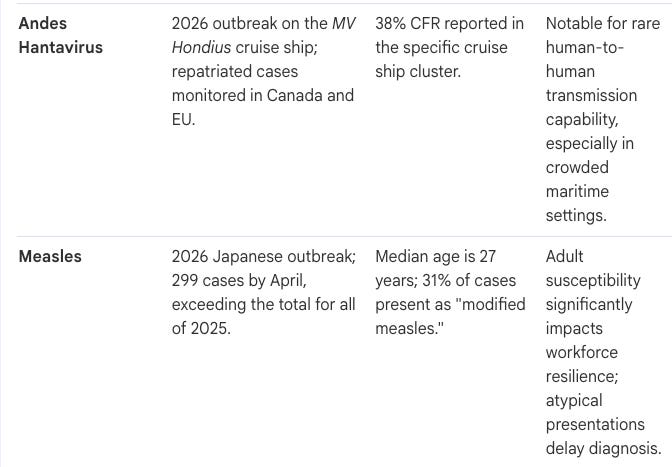
Crisis Management: Coordinated the international response to the 2026 Andes hantavirus outbreak on the MV Hondius cruise ship, which saw a 38% case fatality ratio.
3.4 Japan: Institutional Reform and MCM Strategy
Japan is working to overcome a “Panic and Neglect” cycle through permanent institutional changes.
CAICM: The Cabinet Agency for Infectious Disease Crisis Management provides high-level coordination across ministries.
Revenue Assurance: Piloting revenue-guarantee systems for antibiotics and critical vaccines to maintain production capacity during “peacetime.”
Clinical Trial Acceleration: Setting a goal for 80% of multicenter clinical trials to undergo a single-IRB review by 2034.
3.5 China: Healthy China 2035
China’s strategy is integrated into its 15th Five-Year Plan (2026–2030).
Tuberculosis (TB) Elimination: Aims to reduce incidence to below 43 per 100,000 by 2030, using mRNA vaccines and preventive screening for 80% of close contacts.
Notifiable Diseases: In February 2026 alone, China reported 852,909 cases of notifiable diseases, primarily influenza, viral hepatitis, and COVID-19.
--------------------------------------------------------------------------------
IV. Critical Pathogens and 2026 Outbreak Reports
4.1 Avian Influenza (H5N1 and H9N2)
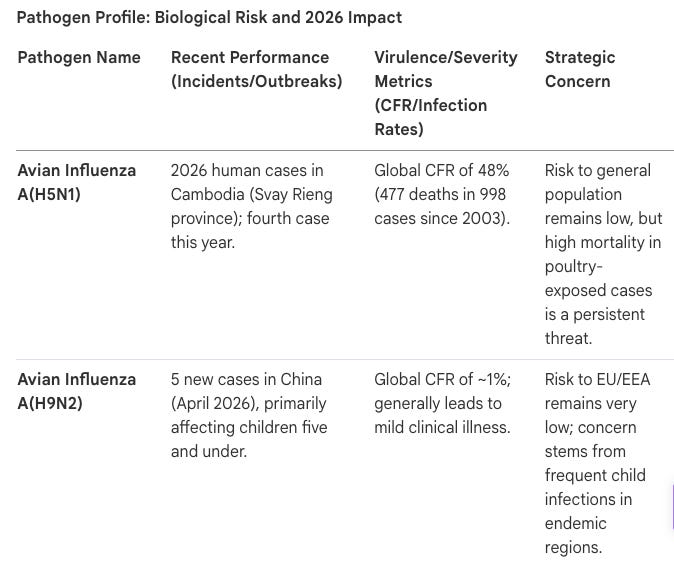
Cambodia (H5N1): A new human case in an adult woman was reported in April 2026. Cambodia has a 56% Case Fatality Rate (CFR) for H5N1 since 2003.
China (H9N2): Five new human cases were reported in early 2026, primarily in children aged five and younger.
4.2 Measles (Japan)
Japan is experiencing its highest measles case count since the COVID-19 pandemic.
Transmission: 299 cases reported by April 2026, surpassing the 2025 total.
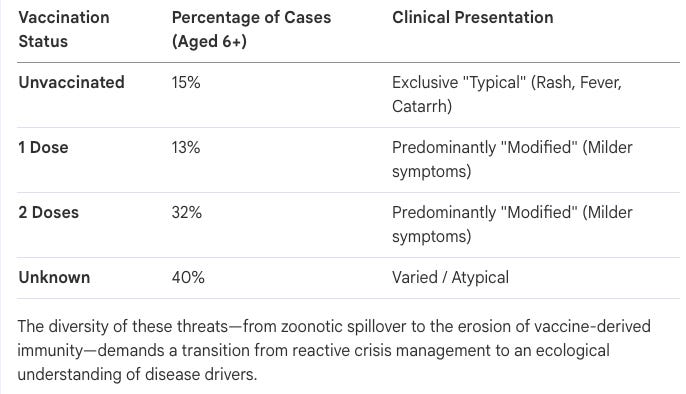
Clinical Presentation: 31% of cases present as “modified measles” (atypical symptoms), which may delay diagnosis.
Immunity Gaps: 40% of patients have an unknown vaccination status, and 32% have received two doses, indicating potential shifts in susceptibility.
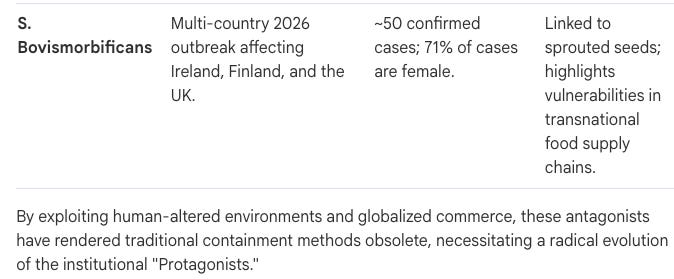
4.3 Salmonella Bovismorbificans (Multi-country)
A 2026 outbreak across at least six EU/EEA countries and the UK has been linked to sprouted seeds and microgreens. All cases are adults, and 71% are female.
--------------------------------------------------------------------------------
The “100-Day Mission”
Spearheaded by the G7 and organizations like CEPI, this goal aims to develop a vaccine within 100 days of identifying a new threat. South Korea conducted a landmark pandemic simulation in February 2026 to test regulatory and manufacturing bottlenecks for this mission.
Quiz & Answer Key
Instructions: Answer the following questions in two to three sentences, ensuring all facts are derived from the provided source context.
According to recent meta-analyses, what is the single greatest environmental driver of infectious disease outbreaks? Researchers have identified biodiversity loss as the primary environmental driver of infectious disease outbreaks, surpassing even climate change and the introduction of non-native species. The loss of species diversity tends to increase the prevalence and severity of diseases in plant, animal, and human hosts by removing natural ecological buffers.
Explain the “dilution effect” hypothesis in the context of zoonotic diseases. The dilution effect suggests that high biodiversity reduces the risk of disease transmission because vectors have a wider variety of animal hosts to feed upon, many of which are “dead-end” hosts that do not carry human pathogens. When biodiversity is lost, these dead-end hosts disappear, leaving only generalist species that are often the most competent reservoirs for zoonotic diseases.
What significant challenge did the Public Health Agency of Canada face regarding its avian influenza vaccine inventory in 2026? By March 2025, the agency secured 870,000 doses of an avian influenza vaccine for high-risk populations, but over 95% of these doses expired unused by February 2026. This has led to recommendations that future procurement be based on more updated risk assessments, cost-benefit analyses, and demand forecasting.
How does warming surface temperature specifically affect the transmission of vector-borne diseases like dengue and malaria? Higher temperatures increase the metabolic and reproductive rates of cold-blooded vectors and accelerate the “extrinsic incubation period,” which is the rate at which a pathogen develops within the vector. This allows mosquitoes and ticks to become infectious faster, leading to more rapid and widespread transmission cycles.
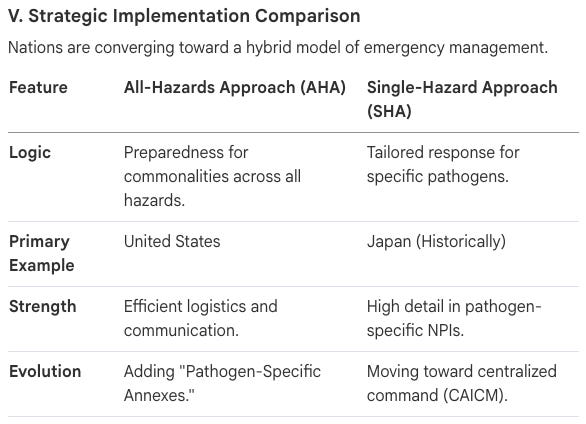
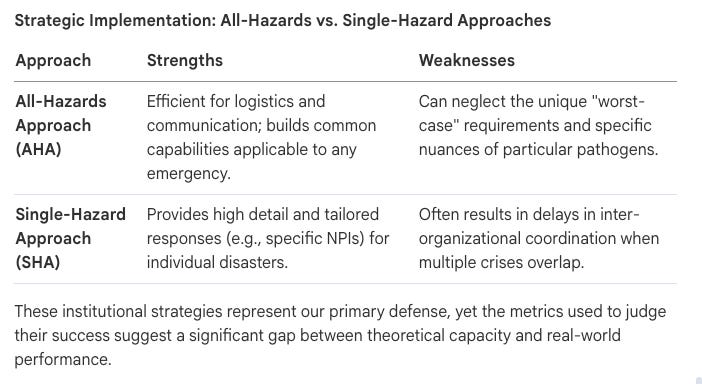
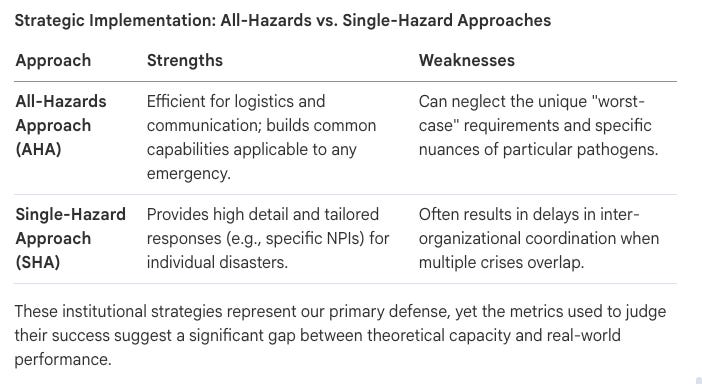
Compare the All-Hazards Approach (AHA) and the Single-Hazard Approach (SHA) to health security. The AHA, used primarily by the United States, focuses on building common capabilities (logistics, communication) applicable to any emergency, while the SHA, historically favored by Japan, creates highly detailed responses for specific pathogens. In 2026, most nations are moving toward a hybrid model to combine general resilience with specific expertise.
What unique characteristic of the Andes hantavirus made the 2026 cruise ship outbreak particularly concerning for health authorities? The Andes hantavirus is concerning because it has a documented ability for limited human-to-human transmission, which is rare among hantaviruses. This necessitated strict infection prevention and control (IPC) protocols and extensive contact tracing during the outbreak linked to the MV Hondius.
Identify the findings of the 2021 Global Health Security (GHS) Index regarding world preparedness. The 2021 GHS Index found that no country is fully prepared for future epidemic or pandemic threats, with a global average score of only 38.9 out of 100. Furthermore, 155 out of 195 countries had not allocated national funds within the previous three years to improve their capacity to address epidemic threats.
What institutional reform did Japan implement in 2023 to coordinate its infectious disease response? Japan established the Cabinet Agency for Infectious Disease Crisis Management (CAICM) in September 2023 to serve as a permanent leadership organization. This agency is designed to oversee and coordinate high-level responses across various ministries, moving away from temporary task forces to ensure institutional permanence.
Describe the significance of “modified measles” as observed in the 2026 Japan outbreak. Modified measles presents with only one or two typical symptoms (rash, fever, or catarrh) and is predominantly found in individuals who have received one or two doses of the vaccine. These atypical presentations are significant because they can delay diagnosis and hinder efforts to control community-level transmission.
What is the “100-Day Mission” and how was it tested in South Korea in 2026? The 100-Day Mission is a G7-endorsed goal to develop a safe and effective vaccine within 100 days of identifying a new pandemic threat. In February 2026, South Korea conducted a landmark tabletop simulation involving the KDCA and private biotech sectors to identify bottlenecks in the vaccine development and licensure chain.
--------------------------------------------------------------------------------
Answer Key
Biodiversity loss; it is the most significant environmental driver, followed by climate change and non-native species.
Dilution effect; high diversity provides more non-competent hosts for vectors, reducing the likelihood of pathogens reaching humans.
Vaccine waste; 870,000 doses were purchased, but over 95% expired unused by February 2026 due to poor demand forecasting.
Extrinsic incubation period; warmer temperatures make pathogens develop faster inside vectors and increase vector reproductive rates.
AHA vs. SHA; AHA is for general resilience; SHA is pathogen-specific. Modern trends favor a hybrid of both.
Human-to-human transmission; Andes hantavirus can spread between people, unlike most other hantaviruses, increasing the risk in crowded settings.
Unpreparedness; the average score is 38.9, and most countries lack dedicated funding or emergency plans for vulnerable populations.
CAICM; it provides a permanent leadership structure to overcome the “panic and neglect” cycle in Japanese health policy.
Atypical presentation; it occurs in vaccinated people and makes surveillance difficult because symptoms are milder or incomplete.
Rapid vaccine development; South Korea used a tabletop exercise to simulate a “Disease X” scenario to test regulatory and manufacturing readiness.
Essay Questions
Instructions: These questions are intended for deeper analysis. Use the themes found in the Source Context to construct your arguments. (No answers provided).
The Convergence of Environmental and Health Policy: Discuss the implications of the finding that biodiversity loss and climate change are the primary drivers of infectious disease outbreaks. How should this scientific consensus influence national health security strategies?
The Crisis of Preparedness vs. Execution: Despite the United States and Canada ranking high on the GHS Index, both countries faced significant challenges in 2026 (e.g., vaccine management in Canada, public trust in the US). Analyze why theoretical capacity often fails to correlate with mortality outcomes and effective response.
Institutionalizing “One Health”: Using Canada and the European Union as examples, evaluate the strengths and weaknesses of the “One Health” approach in managing multi-country threats like avian influenza and hantavirus.
Technological Innovation in Surveillance: Examine the role of Advanced Molecular Detection (AMD), wastewater surveillance, and real-time data modernization in the 2026 strategies of the CDC and the European “BE READY” partnership.
Managing Endemic Threats in East Asia: Compare China’s “Healthy China 2035” goals for tuberculosis elimination with Japan’s response to the 2026 measles outbreak. How do these strategies reflect their respective socio-political environments?
Glossary of Key Terms
Term
Definition
100-Day Mission
A global initiative endorsed by the G7 to prepare the capability to develop safe and effective vaccines within 100 days of a new pandemic threat.
All-Hazards Approach (AHA)
A management strategy focusing on core capabilities (e.g., logistics, triage) that can be applied to any emergency, regardless of the cause.
Andes Hantavirus
A hantavirus species capable of human-to-human transmission, associated with severe respiratory illness and high case fatality rates.
ASHRAE Standard 241
An international standard for the control of infectious aerosols in buildings through enhanced ventilation and filtration.
BE READY
A 2026 European partnership aimed at strengthening the pandemic preparedness research ecosystem across 27 countries.
CAICM
Cabinet Agency for Infectious Disease Crisis Management; Japan’s permanent body for coordinating high-level pandemic responses.
Dilution Effect
The theory that high biodiversity reduces pathogen transmission risk by providing numerous non-competent hosts for disease vectors.
Disease X
A placeholder term used by health organizations to refer to a currently unknown pathogen that could cause a serious international epidemic.
Extrinsic Incubation Period
The time required for a pathogen to develop and become transmissible within a cold-blooded vector after it has been acquired.
GHS Index
The Global Health Security Index; a comprehensive assessment of 195 countries’ health security and preparedness capacities.
One Health
An integrated approach that recognizes the interconnection between the health of people, animals, and their shared environment.
Zoonotic Spillover
The transmission of a pathogen from a vertebrate animal to a human, often facilitated by land-use changes or biodiversity loss.
Cast of Characters
The Cast of Global Health Security: A 2026 Strategic Profile
1. THE STAGE MANAGERS: ENVIRONMENTAL AND SYSTEMIC DRIVERS
In the current global security landscape, infectious disease outbreaks have transitioned from being perceived as sporadic, isolated crises to being recognized as chronic, systemic features of our environment. This strategic shift acknowledges that the rising frequency and severity of pathogenic events are not random, but rather the orchestrated result of deep-seated anthropogenic changes to the Earth’s ecological and social structures. We are no longer merely responding to biological “accidents”; we are managing a theater of risk where environmental and systemic “Stage Managers” dictate the terms of engagement through a vicious cycle of interconnectivity. Climate change and chemical pollution drive habitat loss, which in turn accelerates biodiversity loss, creating a feedback loop of vulnerability.
The primary drivers transforming our natural landscapes into high-risk theaters for zoonotic spillover include:
Biodiversity Loss (The Dilution Effect): The erosion of species variety acts as a catalyst for disease spread. High-biodiversity ecosystems often contain “dead-end” hosts that are poor reservoirs for pathogens. As these species vanish, they are replaced by generalist species—such as specific rodents and birds—that are highly competent reservoirs. The loss of these ecological buffers ensures that pathogens are more likely to find a viable path to human populations.
Climatic Forcing: Climate change serves as a potent force multiplier by dissolving the environmental boundaries that once constrained pathogens. As global surface temperatures rise, disease-carrying vectors like mosquitoes and ticks expand into higher latitudes and altitudes. Warming conditions accelerate the metabolic and reproductive rates of these vectors while shortening the extrinsic incubation period of pathogens, allowing for more rapid transmission cycles.
Urban Connectivity: The integration of global travel and commerce ensures that a localized spillover event can become a global pandemic within months. Air travel effectively neutralizes geographical distance, allowing pathogens to traverse continents faster than their typical incubation periods.
The strategic “So What?” of urbanization reveals a complex dual-reality. While high-density urban environments act as catalysts for the rapid transmission of airborne infections, they can counter-intuitively decrease overall disease risk in specific contexts. Prof. Jason Rohr’s research highlights that urbanization often offers superior sanitation and health infrastructure that rural environments lack, provided the “human shield” effect of infrastructure is maintained. However, the concentration of people creates a high-stakes vulnerability; when infrastructure fails, these dense clusters facilitate explosive spread.
As these environmental stage managers continue to compress the barriers between wildlife and human society, a new cast of biological actors has claimed the spotlight.
2. THE ANTAGONISTS: PROFILE OF EMERGING AND RE-EMERGING PATHOGENS
The contemporary “epidemiological shift” is defined by a dual threat: the looming specter of “Disease X”—unidentified novel threats—and the re-emergence of known virulent agents. These pathogens are increasingly capable of bypassing traditional ecological buffers to strike human populations with higher severity and wider geographic reach.
3. THE PROTAGONISTS: NATIONAL STRATEGIES AND GLOBAL GUARDIANS
National health security is undergoing a critical evolution, moving away from reactive management toward proactive, genomic-led frameworks. Modern strategies prioritize real-time data, “One Health” philosophies, and centralized command structures to anticipate threats before they achieve pandemic scale.
The strategic implementation models of major global actors reveal distinct operational philosophies:
The United States: Operates under the “Moving Forward” initiative, focusing on core data strength and scientific readiness. The Public Health Data Strategy (PHDS) 2026 utilizes an All-Hazards Approach (AHA) to synthesize information from AI and automated FHIR-based data systems.
Japan: Shifting toward centralized command with the Cabinet Agency for Infectious Disease Crisis Management (CAICM). A critical strategic metric is the “Single-IRB” target: ensuring that more than 80% of multicenter clinical trials undergo a unified ethical review within eight years from 2026.
The European Union: Employs the “BE READY” partnership to integrate research into preparedness. Transnational crisis management is spearheaded by HERA, focusing on the procurement of medical countermeasures for cross-border threats.
Canada: While a leader in “One Health” integration (exemplified by H5N1 surveillance in species like the Whooping Crane), the nation faces a severe “Risk Assessment vs. Procurement” gap. This is evidenced by the fact that 95% of 870,000 avian influenza vaccine doses expired unused by February 2026.
China: Under the “Healthy China 2035” initiative, the 15th Five-Year Plan prioritizes TB elimination. Specific “Preventive Treatment Coverage” targets have been set at 60% of close contacts by 2025, rising to 80% by 2030, marking a shift toward proactive care.
4. THE CRITICS: EVALUATING PREPAREDNESS THROUGH METRICS
A troubling paradox has emerged: the disconnect between theoretical preparedness—such as GHS Index scores—and actual mortality outcomes during biological crises. High technical capacity does not guarantee safety if systemic social and political vulnerabilities remain unaddressed.
The 2021–2026 data identifies Four Critical Gaps in global preparedness:
Investment Neglect: 155 out of 195 countries failed to allocate national funds for improving epidemic capacity within the last three years, despite the lessons of COVID-19.
The Risk Environment: Political instability and low public confidence (reported in 161 countries) are major impediments. For non-island nations, the “Risk Environment” score is the most accurate predictor of survival: a 10-point increase in this score correlates to exactly 26.7 fewer deaths per 100,000 people.
Vulnerable Populations: Only 33 countries have overarching emergency plans that specifically consider marginalized sectors, leaving massive populations exposed.
Health System Stagnation: 70% of countries show insufficient capacity in clinics and hospitals, coupled with a chronic shortage of healthcare workforce strategies.
Geography has proven to be a decisive, if temporary, factor. For “Island Nations,” isolation and border control were more impactful than internal security scores. However, geographic isolation is not a strategy—it is a temporary reprieve that must be utilized to build permanent resilience.
5. THE NEXT ACT: STRATEGIC RECOMMENDATIONS FOR BIOLOGICAL RESILIENCE
The era of viewing biological threats as periodic interruptions has ended; we have entered an age of constant, systemic risk. Achieving true “Biological Resilience” requires moving from temporary task forces to permanent, integrated systems of defense.
To secure our future, the following strategic commands must be implemented:
Modernize the Script: Implement interoperable, real-time data systems. Automated FHIR-based data reporting must become the global standard to eliminate regional blind spots in surveillance.
The 100-Day Mission: Prioritize the G7 goal of vaccine development within 100 days. This requires regular, large-scale “fictional pandemic” simulation exercises, modeled after South Korea’s landmark February 2026 exercise, to eliminate bottlenecks in the vaccine chain.
Revenue Assurance: Fix market failures for medical countermeasures through revenue-guarantee pilots. We must utilize proof-of-concept models like the Japanese pilot for Shionogi’s Cefiderocol to ensure production capacity during “peacetime.”
Engineering the Setting: Integrate ASHRAE Standard 241 into national building codes. Managing infectious aerosols must be treated as a matter of critical infrastructure, ensuring minimum requirements for ventilation and filtration are met in all public spaces.
Global security rests on the pivot from temporary task forces to permanent institutional command. Our success will be defined not by our reaction to the next crisis, but by the structural leadership we establish today.
FAQ
As of 2026, the global security environment has undergone a paradigm shift, where infectious disease outbreaks have transitioned from sporadic public health crises to chronic, systemic features of the international landscape. This “new normal” is driven by anthropogenic compression—the rapid erosion of barriers between wildlife, livestock, and dense human populations. For high-level stakeholders, these pathogens represent not merely clinical challenges, but existential threats to economic stability and national resilience that require immediate, proactive integration into security frameworks.
--------------------------------------------------------------------------------
1. The Current Landscape of Viral and Bacterial Threats
What are the primary characteristics and current risks associated with Avian Influenza A(H5N1) and A(H9N2)?
In 2026, avian influenza continues to dominate the global risk profile due to its high mortality and genomic plasticity. While sustained human-to-human transmission remains a theoretical “Disease X” threshold, the spillover dynamics have reached a critical state.
Global H5N1 Status: Since 2003, 998 confirmed human cases have been recorded across 25 nations, with 477 deaths resulting in a Case Fatality Rate (CFR) of 48%.
Genomic Nuance (Cambodia): In April 2026, a woman in her 60s tested positive for Clade 2.3.2.1e, which is currently circulating in regional poultry. Cambodia’s specific CFR remains alarmingly high at 56% (52 deaths out of 93 total cases).
Sentinels and Compensation (Canada): Canada reported its first domestically acquired human case in British Columbia in 2025. Between 2021 and 2026, HPAI has been detected in every province, impacting 43 bird species. Crucially, detections in the Whooping Crane (population estimated at only ~550) serve as a vital sentinel for species-at-risk surveillance.
H9N2 Comparative Risk: In early 2026, China reported five new pediatric cases. While Southeast Asia remains a monitorable hotspot due to high poultry interaction, the historical CFR is only 1%. The ECDC currently assesses the risk to the general population in the EU/EEA as “very low.”
What is the significance of the 2026 Andes hantavirus outbreak on the cruise ship MV Hondius?
The May 2026 incident involving the MV Hondius was a watershed moment for maritime biosecurity. Following a cluster of severe respiratory illnesses, the UK notified the WHO, triggering a multi-continental response. The outbreak exhibited a 38% case fatality ratio, but its primary significance lies in the Andes virus’s unique capacity for human-to-human transmission, specifically during the early high-viral-load phase. This event necessitated complex international coordination for medical evacuations, with patients transported to specialized facilities in the Netherlands and South Africa, highlighting the need for standardized global disembarkation protocols.
How has the 2026 measles outbreak in Japan challenged established immunity assumptions?
The 2026 outbreak in Japan, featuring genotypes B3 and D8, has signaled a shift toward established community-level transmission. A major clinical challenge is the rise of “modified measles”—atypical presentations (1–2 symptoms like mild fever or isolated rash) that escape standard surveillance, delaying diagnosis.
--------------------------------------------------------------------------------
2. Environmental and Anthropogenic Drivers of Disease
Environmental degradation serves as the primary “force multiplier” for pathogenic expansion. By 2026, it is evident that the erosion of natural barriers is the fundamental engine driving the increased frequency of zoonotic spillovers.
To what extent does biodiversity loss drive infectious disease outbreaks compared to other factors?
A 2024 meta-analysis in Nature confirmed that biodiversity loss is the single greatest environmental risk factor for outbreaks. This is dictated by the “dilution effect”: high-biodiversity ecosystems contain diverse “dead-end” hosts that disrupt transmission. As specialized species are lost, they are replaced by hardy “generalist” reservoirs (e.g., specific rodents) that are highly competent at harboring and transmitting zoonotic pathogens to humans.
How is climate change specifically altering the “environmental envelopes” of pathogens and vectors?
Climate change fundamentally recalibrates the biological parameters of disease transmission:
Vector-Borne Diseases: Warmer temperatures increase the metabolic rates of ectotherms (mosquitoes, ticks) and significantly shorten the extrinsic incubation period—the time required for a pathogen to become infectious within the vector—accelerating transmission cycles.
Water-Borne Diseases: Rising sea temperatures expand the range of pathogens like Vibrio cholerae. The warming of brackish waters has facilitated the northward expansion of Vibrio and Shewanella infections into the Baltic and North Seas (e.g., Denmark).
Zoonotic Displacement: Extreme weather (floods/droughts) displaces wildlife and humans into shared ecological niches, creating high-probability spillover environments.
What role does urbanization and human movement play in 2026 disease dynamics?
Urbanization offers a “sanitation advantage” through infrastructure but creates high-density environments where airborne transmission is optimized. Global air connectivity ensures that a local spillover can achieve pandemic status within months, bypassing traditional incubation-period buffers.
Critical Takeaways on Social Vulnerability:
Poverty and Vulnerability: Lack of shelter and nutrition lowers individual immunological thresholds.
Infrastructure Fragility: High-density, under-resourced urban areas lack the “sanitation advantage,” leading to explosive water-borne and respiratory spread.
Translational Inequity: National wealth dictates the speed of response, leaving impoverished populations as permanent reservoirs for endemic pathogens.
These ecological shifts have made standardized national preparedness metrics more critical than ever, leading into an evaluation of global security benchmarks.
--------------------------------------------------------------------------------
3. Benchmarking Global Health Security (GHSI & JEE)
Standardized metrics, specifically the GHS Index (GHSI) and the Joint External Evaluation (JEE), are vital for identifying systemic vulnerabilities. These metrics allow for a shift from “theoretical capacity” to “execution strategy.”
What does the 2026 GHS Index reveal about the current state of global preparedness?
The 2026 GHSI data confirms a state of global stagnation. The average global score remains at 38.9, and no country has achieved the “top tier” (scores > 80), indicating that even the most advanced nations possess significant gaps in their biosecurity frameworks.
Top 10 Ranked Countries (GHSI 2026):
United States (75.9)
Australia (71.1)
Finland (70.9)
Canada (69.8)
Thailand (68.2)
Slovenia (67.8)
United Kingdom (67.2)
Germany (65.5)
South Korea (65.4)
Sweden (64.9)
Why did high preparedness scores fail to correlate with COVID-19 mortality outcomes?
The “COVID-19 Paradox” revealed that technical capacity is secondary to two factors:
The Risk Environment: Technical readiness is ineffective without political stability and public trust. Nations with low “Risk Environment” scores faced a breakdown in MCM (Medical Countermeasure) uptake.
Demographic Determinants: The percentage of the population aged 65 and above was a significantly stronger predictor of mortality than GHSI scores, necessitating a move toward demographically-targeted resilience.
These metrics are now being utilized to refine national execution strategies, moving toward more integrated policy models.
--------------------------------------------------------------------------------
4. National Execution Strategies and Policy Models
The 2026 landscape is defined by a shift toward “One Health” integration, merging human, animal, and environmental surveillance into a singular strategic framework.
How has Canada integrated the “One Health” approach into its management of Avian Influenza?
Canada’s multi-agency response (PHAC, CFIA, ECCC) has been aggressive but faced logistical friction. The CFIA has paid out approximately $360 million in compensation for 17.3 million culled or dead commercial birds. However, a 2026 audit revealed a critical strategic failure: while the government secured 870,000 avian influenza vaccine doses, over 95% of the inventory expired unused in February 2026. This highlights the “Translational Medicine Lag” and the difficulty of peacetime procurement in the absence of accurate demand forecasting.
What are the core pillars of Japan’s institutional reforms under the Cabinet Agency for Infectious Disease Crisis Management (CAICM)?
Japan is attempting to break the “Panic and Neglect” cycle—the historical trend of societal alarm during crises followed by total disinvestment.
Structural Integration: The Japan Institute for Health Security (JIHS) now centralizes NIID and NCGM functions.
Clinical Acceleration: A new “single-IRB” framework aims for 80% of multicenter trials to complete ethical review within a unified system by 2034.
MCM Strategy: Japan is piloting revenue-guarantee systems for antibiotics and vaccines to incentivize private sector production during inter-pandemic periods.
What are the objectives of China’s 15th Five-Year Plan regarding the “Healthy China 2035” initiative?
China has prioritized Tuberculosis (TB) elimination, moving from simple detection to preventive treatment for high-risk cohorts.
What is the “100 Days Mission,” and how is it being tested in 2026?
The CEPI-led “100 Days Mission” aims to develop and license vaccines within 100 days of identifying a novel threat. In February 2026, South Korea conducted a landmark tabletop simulation involving the KDCA and private industry. The exercise was a critical stress test of the vaccine development chain, identifying regulatory and manufacturing bottlenecks that would otherwise delay a “granular and tailored” response to a real-world Disease X.
--------------------------------------------------------------------------------
5. Engineering and Infrastructure Interventions
The final frontier of biosecurity is the built environment. As respiratory pathogens remain the primary pandemic threat, indoor air quality (IAQ) and building codes are now considered primary defense mechanisms.
What is ASHRAE Standard 241, and why is its integration into building codes being petitioned in 2026?
ASHRAE Standard 241 (Control of Infectious Aerosols) establishes minimum requirements for ventilation and filtration to reduce infection risk. Petitioners in 2026 are framing this as an equity issue and a necessary response to the 17-year lag in translational medicine. If medicine takes nearly two decades to move from the laboratory to the bedside, building engineering must provide the immediate protection necessary to safeguard public health and reduce the economic burden of workforce shortages.
How can building retrofits align with broader environmental sustainability goals?
A strategic synergy exists between health and climate resilience. Programs like Canada’s Deep Retrofit Accelerator Initiative (DRAI) allow for the simultaneous installation of energy-efficient heat pumps and Standard 241-compliant ventilation. This “dual-track” approach ensures that building retrofits meet net-zero goals while hardening infrastructure against airborne pathogenic risks.
The Path Toward Biological Resilience
The era of sporadic pathogenic crises has been replaced by a state of permanent, systemic risk. Biological resilience in 2026 requires a total synthesis of “One Health” philosophies—integrating environmental sentinels like the Whooping Crane with high-tech genomic surveillance and robust building engineering. Only through this permanent institutionalization of lessons can we secure durable human and economic security in a warming, interconnected world.
Table of Contents with Timestamps
00:00 — Opening & Mission Statement The Heliox signature opening: independent, moderated, timely conversations about things that matter. An invitation to breathe easy and go deep.
00:24 — The Global X-Ray: May 2026 A woman in Cambodia. Five children in China. A salmonella cluster in Europe. Hantavirus on a cruise ship. Why these seemingly disconnected events alarm the world’s top public health experts—and why a quiet baseline makes them more frightening, not less.
07:52 — The GPMB: Scientists on the Edge Who are the authors of the 2026 Capstone Report, “A World on the Edge”? The origin story of the Global Preparedness Monitoring Board, born from the tragedy of West African Ebola in Guinea, 2013, and their haunting role as Cassandra before COVID-19.
11:15 — The Paradox: Better Tools, Worse Odds Despite mRNA breakthroughs and billions spent, the GPMB concludes pandemic risk is trending the wrong direction. The VUCA world explained—volatile, uncertain, complex, ambiguous—and why sharper tools in trembling hands do not equal safety.
13:32 — The Engine of Outbreaks: One Health and Nature’s Frayed Edges How biodiversity loss, deforestation, and climate change are dismantling the natural buffer zones between animal viruses and human populations. The bat, the pig farm, and the farmer. Zoonotic spillover as infrastructure failure.
18:34 — The Global Scorecard: A Failing Grade An in-depth look at the 2021 Global Health Security Index. A global average of 38.9 out of 100. Seventy-three countries without adequate health systems. Eighty-one percent without wraparound economic support. Why the economy becomes the engine of viral transmission.
24:01 — The Silicon Guardians: Reasons for Hope The pivot from reactive crisis management to institutional permanence. Wastewater genomics in the U.S., the EU’s €1.8 billion BE Ready Partnership, Japan’s Cabinet Agency for Infectious Disease Crisis Management, China’s elevated public health authority, and South Korea’s revolutionary stakeholder mapping approach.
32:32 — The Collapsing Foundation: Trust and Equity Why even the most sophisticated pandemic architecture fails without public trust. Vaccine nationalism, the structural disincentive for developing nations to share outbreak data, and AI as a double-edged sword—miraculous predictor or misinformation accelerant.
36:41 — Three Demands: The GPMB’s Ultimatum The Board’s three priorities for survival: independent risk monitoring with real teeth; equitable access to countermeasures through binding international agreements and decentralized manufacturing; and sustainable financing—including the revolutionary Day-Zero financing concept.
41:32 — Synthesis: The Entire Patient The hosts step back to survey the full journey—from the fractured x-ray of 2026 to the systemic conditions beneath it. Pandemic preparedness as grocery supply chains, inflation rates, and the ability of your neighbour to stay home when sick.
43:55 — Closing & Call to Reflection An essential question for the listener: will we cure the underlying societal conditions before the next small blip on the radar becomes an unstoppable global storm?
44:02 — Credits & Outro Producer credits, the four recurring Heliox narrative frameworks, and an invitation to explore helioxpodcast.substack.com.
Index with Timestamps
4. Index
Adaptive complexity, 44:29
Advanced Molecular Detection (AMD), 25:33
Andes virus, 05:23, 05:28
Anthropogenic risk, 14:01
Avian influenza (H5N1), 03:05, 06:23, 06:36
Avian influenza (H9N2), 03:14, 06:25
BE Ready Partnership, 28:27
Biodiversity loss, 14:06, 42:20
Boundary dissolution, 44:29
Cambodia, avian flu cases, 01:03, 03:05, 06:25
Climate change, 16:14, 42:20
Cruise ship hantavirus cluster, 01:06, 03:24, 05:39
Day-Zero financing, 39:30, 40:34, 41:01
Deforestation, 15:15, 37:26
Disease X, 17:44
Ebola, West African epidemic, 02:07, 08:23, 09:03, 10:59
Ecological buffer zones, 14:30
Economic wraparound services, 22:21
Embodied knowledge, 44:29
Engine of outbreaks, 13:41, 18:14
Equity, 34:28, 35:11
European Centre for Disease Control (ECDC), 01:33
European Union (BE Ready Partnership), 28:15
Generative AI and misinformation, 36:20
Global Health Security Index (GHS Index), 18:34, 20:04, 42:13
Global Preparedness Monitoring Board (GPMB), 01:45, 07:54, 08:09, 09:35, 11:10, 32:32, 36:34, 37:43
Hantavirus, 03:24, 04:39, 05:03, 05:30
Human-to-human transmission, 05:01, 05:30, 06:54
Japan, Cabinet Agency for Infectious Disease Crisis Management (CAICM), 29:36
Meliandu, Guinea, 08:18
mRNA vaccines, 11:17, 38:34
Mosquitoes, disease range expansion, 16:40
National Disease Control and Prevention Administration (China), 30:18
One Health philosophy, 16:50, 17:19, 37:33, 43:02
Pandemic financing, 38:47, 38:55, 39:08
Pathogen Access and Benefit Sharing System (PABS), 37:50
Political insecurity, 20:30, 21:01
Public health data strategy, 25:25
Quantum-like uncertainty, 44:29
Radar analogy (drones/perimeter), 04:22, 06:14, 43:52
Risk environment category (GHS Index), 20:04
SARS-CoV-2, 04:03, 10:24, 26:38
Silicon Guardians, 24:24, 42:04, 32:39
South Korea, stakeholder mapping, 30:57, 31:10, 31:47
Sustainable financing, 38:42, 38:47
Traveler-based Genomic Surveillance (TGS), 27:35, 27:41
Trust, erosion of, 02:33, 32:51, 33:04, 34:00
Tuberculosis, China surveillance, 30:37
Vaccine nationalism, 34:06, 34:11
VUCA world, 11:37, 11:47
Wastewater surveillance, 25:49, 26:29, 26:54, 42:04
World Health Assembly, 37:09
World Health Organization (WHO), 01:33, 09:35, 30:38
Zoonotic spillover, 15:35, 15:48, 16:04
Poll— Global Pandemic Risk We’d love your take on three big
Post-Episode Fact Check— “Global Pandemic Risk Is Still Increasing”
Claim: A woman in her 60s and a child aged 5 and 1 contracted avian influenza in Cambodia after contact with sick poultry. Assessment: Plausible and consistent with documented H5N1 spillover patterns in Cambodia. WHO regularly reports sporadic human H5N1 cases in Cambodia, particularly in rural poultry-contact settings. ✅ Consistent with known reporting patterns.
Claim: Five human cases of H9N2 in China, four of them children under five. Assessment: H9N2 human infections are periodically reported in China by the WHO, predominantly in young children. The age distribution described matches historical case patterns. ✅ Consistent with documented H9N2 epidemiology.
Claim: A multi-country salmonella outbreak in Europe linked to sprouted microgreens. Assessment: Microgreens and sprouts have been documented as salmonella outbreak vehicles in multiple European incidents. The specific 2026 cluster described cannot be independently verified from training data but is plausible. ⚠️ Plausible; specific 2026 event unverified against external sources.
Claim: The Andes virus has documented limited human-to-human transmission. Assessment: Accurate. The Andes hantavirus, endemic to Argentina and Chile, is the only hantavirus with documented, albeit limited, human-to-human transmission. ✅ Scientifically accurate.
Claim: The historical fatality rate for H5N1 in humans is approximately 48 percent. Assessment: WHO’s cumulative data on confirmed H5N1 cases has historically shown a case fatality rate around 50–60%. The 48% figure is within the documented range, though CFR estimates vary by surveillance context. ✅ Broadly accurate.
Claim: The GPMB was co-convened by the WHO and the World Bank Group in 2018. Assessment: Accurate. The Global Preparedness Monitoring Board was established in 2018 as an independent body co-convened by the WHO and World Bank. ✅ Accurate.
Claim: The GPMB’s first annual report was published in September 2019 and warned of vulnerability to a fast-moving respiratory pathogen. Assessment: Accurate. The GPMB’s September 2019 report, titled “A World at Risk,” explicitly warned that the world was acutely vulnerable to a global respiratory pandemic. ✅ Accurate.
Claim: The West African Ebola epidemic resulted in over 28,000 recorded cases and more than 11,000 deaths.Assessment: Accurate. WHO figures for the 2014–2016 West African Ebola epidemic documented approximately 28,616 cases and 11,310 deaths. ✅ Accurate.
Claim: The 2021 Global Health Security Index global average score was 38.9 out of 100. Assessment: Accurate. The 2021 GHS Index report published an overall global average score of 38.9. ✅ Accurate.
Claim: 81 percent of countries do not provide wraparound services during a health crisis. Assessment: This figure is cited in the 2021 GHS Index under indicators for socioeconomic resilience. ✅ Consistent with published GHS Index data.
Claim: 93 percent of countries have some form of paid medical leave, but nine upper-middle and high-income countries, including the United States, do not provide universal paid sick leave at the federal level. Assessment: The U.S. federal government does not mandate universal paid sick leave—accurate as of 2024. The 93% figure and the nine-country exclusion figure are consistent with ILO and GHS Index reporting. ✅ Broadly accurate.
Claim: The EU’s BE Ready Partnership involves 81 organizations across 27 countries and is backed by a €1.8 billion investment. Assessment: The BE Ready (Better Preparedness and Readiness) initiative is a real EU-funded program. Specific figures should be verified against current EU project documentation, as program scope may have evolved. ⚠️ Plausible; specific figures warrant confirmation against current EU documentation.
Claim: Japan created the Cabinet Agency for Infectious Disease Crisis Management (CAICM). Assessment: Japan established the Infectious Disease Crisis Management Office at the Cabinet Secretariat level following COVID-19 lessons. The acronym CAICM is used in the episode to describe this structure. ✅ Consistent with documented Japanese health governance reforms.
Claim: China established the National Disease Control and Prevention Administration. Assessment: Accurate. China formally established the National Disease Control and Prevention Administration (NDCPA) in 2023, elevating public health authority. ✅ Accurate.
Claim: Wastewater surveillance can detect viral RNA before symptomatic cases appear, sometimes from asymptomatic individuals. Assessment: Accurate and well-established in peer-reviewed literature. Fecal shedding of SARS-CoV-2 and other viruses precedes symptom onset and occurs in asymptomatic cases. ✅ Scientifically accurate.
Overall Assessment: The episode’s factual claims are well-grounded in published scientific and institutional sources. Two claims — the specific 2026 microgreens outbreak and EU partnership figures — are plausible but could not be independently verified from pre-August 2025 data. All core epidemiological, historical, and institutional claims are accurate and appropriately nuanced.
Image (3000 x 3000 pixels)

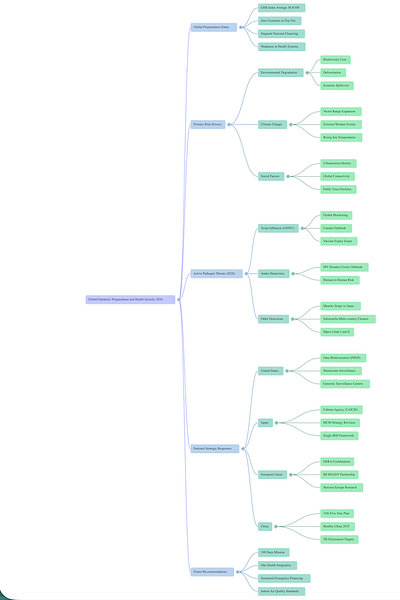
Mind Map
Comic
Street Art
Infographics