👵 The Script We Never Finished Writing
On aging, elderhood, and the third act we abandoned
Third act curtain falls —
Elder, not old: wisdom blooms
where we forgot to look.
With every article and podcast episode, we provide comprehensive study materials: References, Executive Summary, Briefing Document, Quiz, Essay Questions, Glossary, Timeline, Cast, FAQ, Table of Contents, Index, Polls, 3k Image, Fact Check, Comic and
Street Art at the very bottom of the page.
Soundbite
Trailer
Essay
There is a moment, somewhere around your mid-forties, when you start to notice them differently. The older woman on the bus with the arthritic fingers and the cheerful dress. The retired man at the coffee shop nursing a single cup for two hours. You notice them, and then — almost immediately — you look away. Not out of cruelty. Out of something much older and more reflexive than that. Out of the ancient, animal need to say: not yet. Not me.
We have built an entire civilization around that flinch.
Dr. Louise Aronson, a geriatrician at UCSF whose book Elderhood reads like a slow, illuminating reckoning, argues that western medicine — and western society more broadly — has been operating from a fundamentally broken script. We treat human life as a two-act play: childhood, with all its exuberant character development, and adulthood, where the real drama unfolds. And then we simply pretend the third act doesn’t exist, or worse, we treat it as a prolonged, uncomfortable curtain drop. The lights slowly dim. The audience politely waits to leave.
What if we’ve been reading the wrong play entirely?
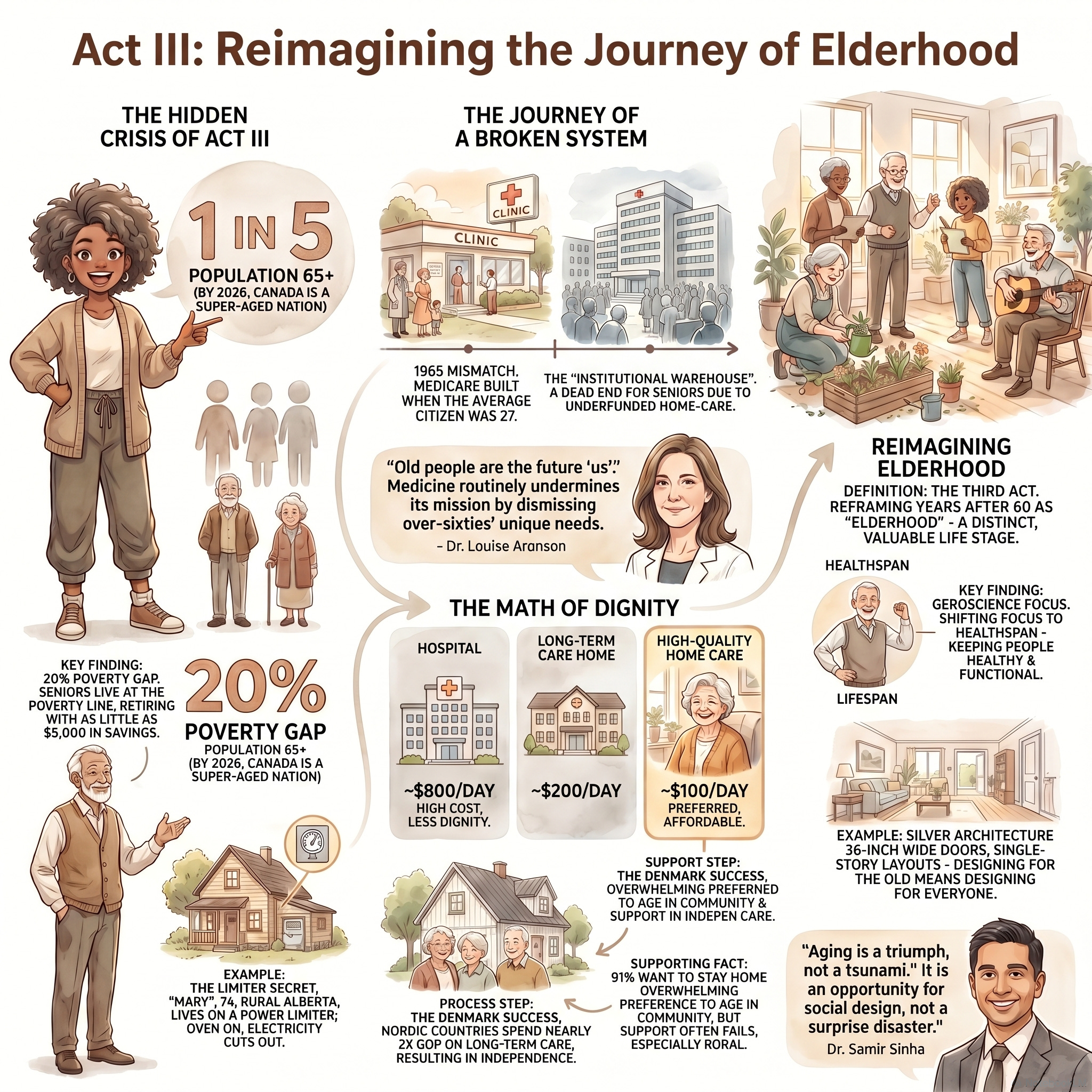
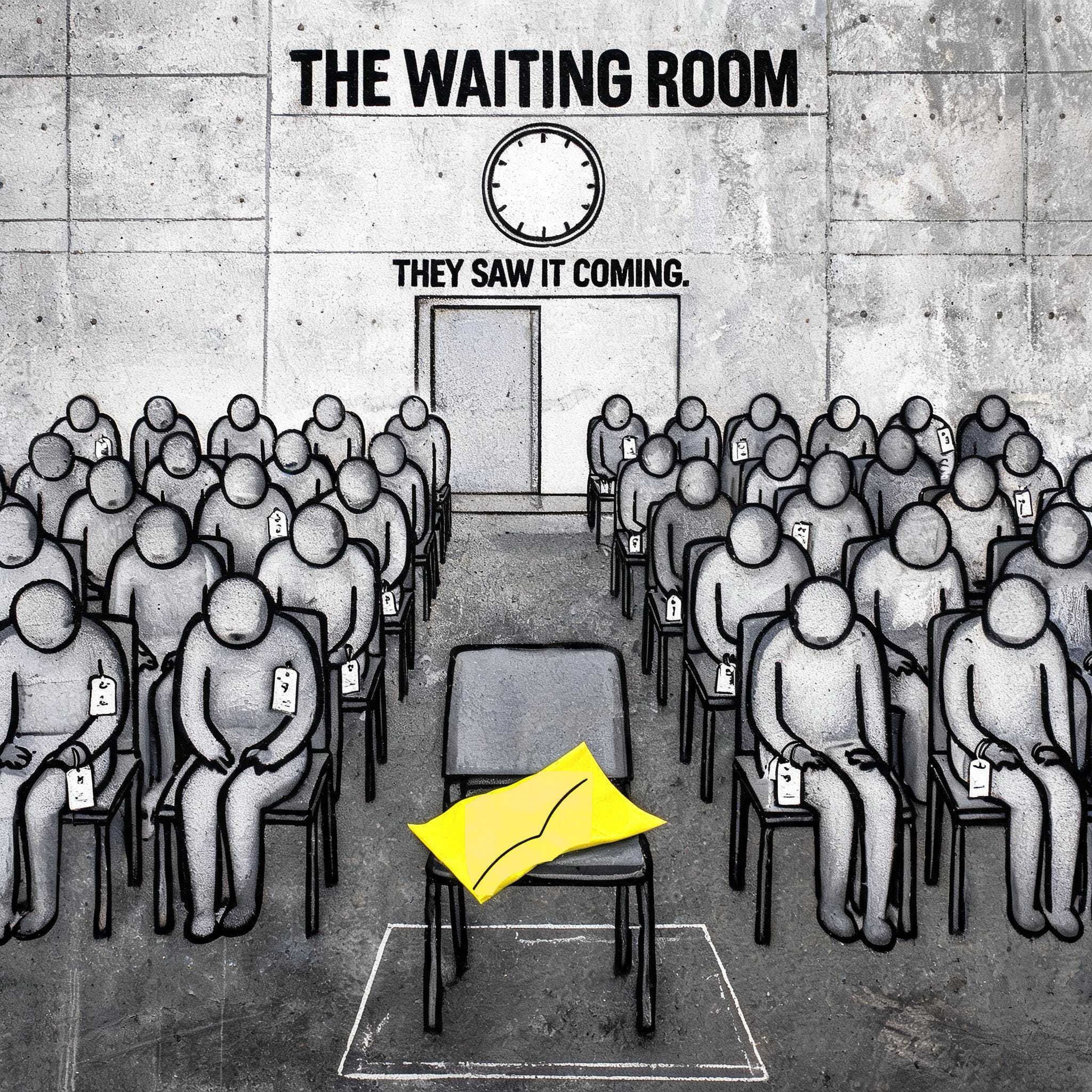
Canada crossed a significant threshold this year. We are now officially a “super-aged” nation — one in five Canadians is over 65. Our hospitals, our cities, our pension systems, our very language, are straining under the weight of a reality we had four decades to prepare for and largely chose to ignore. We saw it coming in the birth rate data. We tracked the boomers year by year. And still we find ourselves caught flat-footed, reaching for inadequate metaphors — “silver tsunami,” that catastrophizing phrase coined in the 1980s, still deployed by politicians and medical journals as though the longevity of millions of human beings is some kind of natural disaster rather than the crowning achievement of modern medicine.
This is where the story gets interesting, and worth sitting with.
A colleague of Aronson’s, a physician named Dr. Mikko, conducts a simple word association exercise with his medical students. He gives them the word “old” and asks them to write whatever comes to mind. The results, without exception, cluster around loss, decline, obsolescence, and disease. Then he changes a single word. He asks them to associate with “elder.” Suddenly the same demographic — the exact same stage of human life — generates words like wisdom, resilience, perspective, and respect. The label, as Aronson writes, literally dictates the value. We have not failed to care for our elders because we are callous. We have failed because we have been using the wrong vocabulary, and vocabulary shapes policy, shapes medicine, shapes architecture, shapes everything that follows.
The practical consequences of this linguistic and psychological failure are not abstract. They are clinical, economic, and occasionally fatal.
The Canadian Institute for Health Information paints a picture that should stop us cold: one in five older Canadians currently lives at or below the poverty line. In the CIHI documentary Aging Without Dignity, we meet Mary, a 74-year-old in rural Alberta whose power company has installed a limiter on her electricity because she cannot pay her bills — a device that restricts current to just enough to prevent pipes from freezing, making her home effectively uninhabitable in winter. She rations toilet paper. She cannot run the microwave and toaster simultaneously. She relies on the charity of neighbors to feed her cat.
We meet Paul, 77, who planned responsibly, trusted his pension, and then watched macroeconomic forces — rental inflation, food costs — quietly eviscerate his safety net. His most heartbreaking line: I have no money after I pay my rent to have fun, and I miss that.
Joy. He misses joy. And that sentence contains, in miniature, everything Aronson is arguing. Dignity in elderhood is not just about biological survival. It requires the autonomy and the resources to experience connection, pleasure, and meaning. To have the lights on. To occasionally run two appliances at once.
Here is the particular cruelty of our current system: it is not only failing older people morally, it is failing economically. The CIHI data reveals that keeping an older adult in an acute care hospital bed while they wait for placement costs roughly eight hundred dollars a day. A long-term care institution runs approximately two hundred. But robust, targeted home care — which is what over 80% of older adults say they desperately want — costs about one hundred dollars a day. We are systematically uprooting people from their communities, stripping them of autonomy, warehousing them in institutions they fear, and paying double the price to do it. The irrationality would be almost comic if its consequences weren’t so devastating.
But here is where the science begins to open doors.
The emerging field of geroscience is mounting a quiet revolution against our assumptions. For most of the twentieth century, medicine was obsessed with lifespan — the accumulation of years, the defeat of acute causes of death. The new frontier is healthspan: the period of life lived free from chronic debilitating disease. Researchers are developing senolytic therapies that target the “zombie cells” — damaged cells that refuse to die and instead secrete inflammatory chemicals that degrade healthy surrounding tissue, driving arthritis, cardiovascular disease, and cognitive decline. If we can clear those cells systematically, we may be able to compress the period of morbidity, allowing people to live into their eighties and nineties with vitality until very near the end.
Meanwhile, demographers like Stanford economist John Chauvin are challenging the very definition of “old.” He proposes that age should be measured not by years lived, but by statistical proximity to death — specifically, when annual mortality risk reaches 2%. By that biological metric, a woman in 1920 was “old” at 55. Today, thanks to advances in medicine and public health, she doesn’t cross that threshold until 73. The biological reality of old age has shifted by nearly two full decades. Yet our mandatory retirement ages, our pension eligibility cutoffs, and our clinical protocols remain anchored to a mid-twentieth century calendar.
We are, in other words, pathologizing people who are biologically in the prime of their later adulthood. We are stripping them of purpose and pushing them to the margins because they’ve hit an arbitrary bureaucratic number that was invented by Industrial Revolution governments to cycle factory workers out of the labor pool. It has no basis in biology.
The remedies Aronson envisions are neither utopian nor prohibitively expensive. “Silver architecture” — designing spaces with acoustic dampening, tactile flooring, high-contrast colors, and indirect lighting — does not require tearing down cities; it requires integrating thoughtful design at the outset rather than retrofitting after the fact. Naturally Occurring Retirement Communities (NORCs) bring specialized healthcare and social services directly into the buildings where older adults already live, rather than building distant institutional facilities and uprooting people to fill them. Denmark has built this distributed model at national scale, and the downstream effect is staggering: they are currently constructing hospitals that are a fraction of the size of Canadian or American hospitals, simply because they eliminated the structural need to use acute care wards as overflow warehousing for seniors.
They solved hospital crowding by fixing elder care in the community.
And then there is the philosophical shift, which may be the hardest and most necessary of all. The concept of “successful aging” — that 1997 metric defining success as maintaining the physiology and engagement level of a middle-aged adult — imposes a brutal pass-fail dynamic on natural human decline. The 90-year-old skydiving posters in hospital lobbies are meant to inspire. What they actually do, Aronson argues, is shame the vast majority of patients experiencing perfectly normal deterioration. They frame ordinary frailty as a character flaw rather than an inevitable biological reality.
Against this, Aronson offers a counter-narrative, quiet and human-scaled. A patient named Inez. Multiple strokes, advanced dementia, entirely bed-bound. By the prevailing metrics: a failure. But Aronson watched her comment on the bright colors of her clothing. Joke in Spanish behind her husband’s back. Raise her eyebrows. Wink.
Joy and meaning, it turns out, do not evaporate the moment a body becomes frail.
The anthropologist Margaret Clark found that elders who thrived were not those desperately clinging to their youth, but those who had consciously adapted: releasing middle-aged metrics of professional status and physical dominance, and embracing instead congeniality, self-acceptance, community, and the sharing of hard-won wisdom. They did not fail at being middle-aged. They succeeded at being elders.
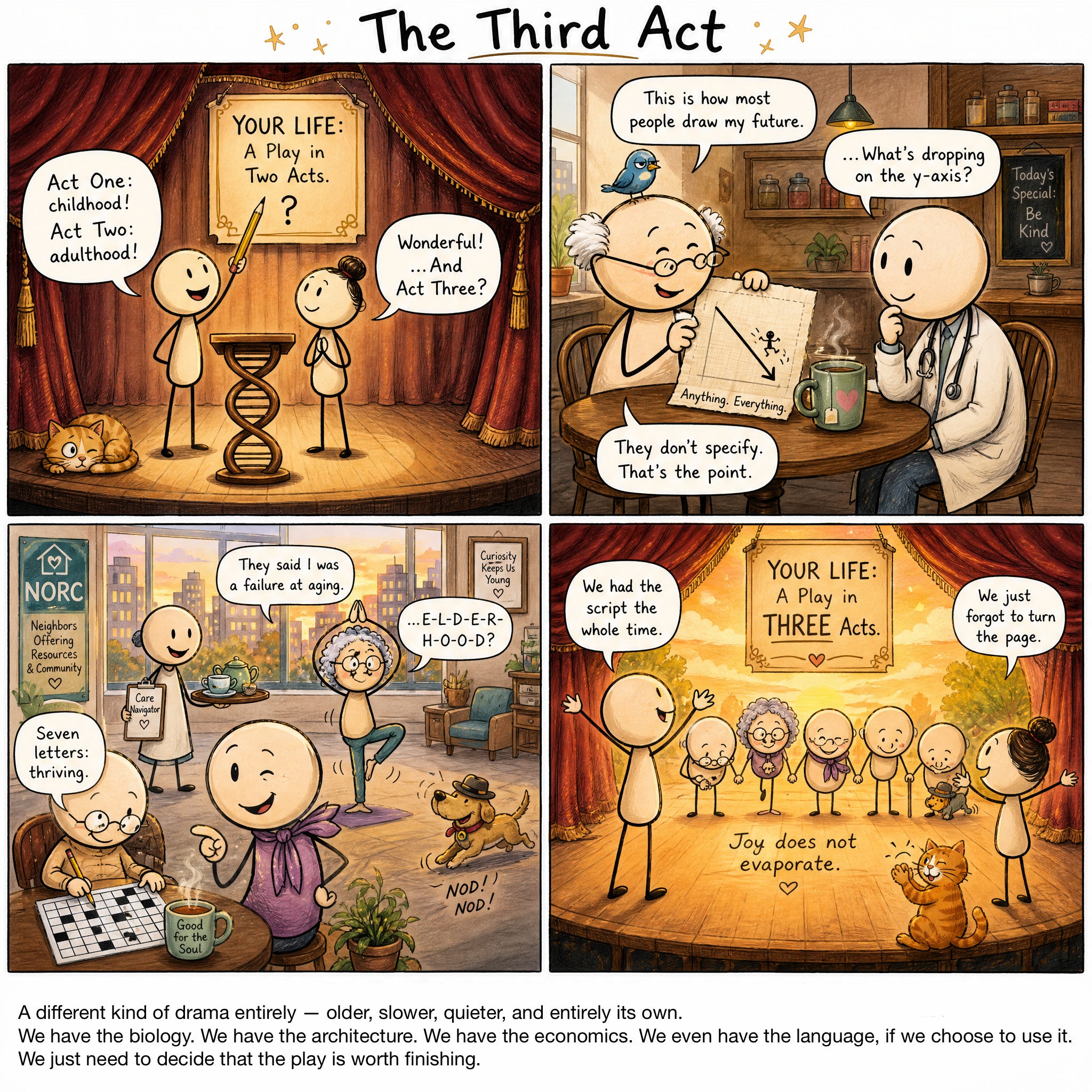
This is the third act we wrote out of the script. Not a slow curtain drop. Not a polite wait to leave the theater. A different kind of drama entirely — older, slower, quieter, and entirely its own.
We have the biology. We have the architecture. We have the economics. We even have the language, if we choose to use it.
We just need to decide that the play is worth finishing.
Heliox: Where Evidence Meets Empathy explores this and related topics at helioxpodcast.substack.com. Produced by Michelle Bruecker and Scott Bleackley.


Link References
Elderhood: Redefining Aging, Transforming Medicine, Reimagining Life
The National Imperative of an Aging Society: Demographics, Geroscience, and the Transformation of Later Life in Canada
Perspectives on Growing Older in Canada: The 2025 NIA Ageing in Canada Survey | Manulife
Aging Without Dignity: Seniors and Poverty | CIHI
Aging in the 21st Century: the Triumph and the Challenge - Rapport - Western University
CIHR Institute of Aging Strategic Plan 2023-2028 - CIHR
Aging in a Vertical City - NORC Innovation Centre
A science-based solution to help older Canadians age in place - CIHR
8 Trends That Transformed Canadian Healthcare in 2025 - Serefin
Age-Friendly Communities - Canada.ca
AGE-WELL | Canada’s technology and aging network
Population Projections for Canada (2025 to 2075), Provinces and Territories (2025 to 2050)
Canada Population Pyramid 2025 - Demographics & Birth Statistics
Published plans and annual reports 2025–2026: Ministry of Long-Term Care | ontario.ca
Published plans and annual reports 2024–2025: Ministry of Long-Term Care | ontario.ca
Targeting Cellular Senescence for Healthy Aging: Advances in Senolytics and Senomorphics - PMC
2025 Catalyst Grant: Analysis of Canadian Longitudinal Study in Aging (CLSA) Data - CIHR
Episode Links
Available for broadcast on PRX
Other Links to Heliox Podcast
YouTube
Substack
PRX ( Public Radio Exchange)
Podcast Providers
Spotify
Apple Podcasts
Patreon
FaceBook Group
STUDY MATERIALS
Executive Summary
As of 2026, Canada has officially become a “super-aged” nation, with one in five citizens aged 65 or older. This demographic shift, though long-predicted, has exposed significant gaps in the country’s ability to provide dignified, affordable, and accessible care for its aging population. Current data reveals a crisis of “hidden poverty,” where 20% of seniors live at or below the poverty line, often forced to choose between food, electricity, and housing.
The emerging consensus among geriatric experts and policymakers suggests a critical need to transition away from hospital-centric and institutionalized care toward integrated, community-based models. Comparative data indicates that home-based care is not only preferred by 91% of seniors but is also significantly more cost-effective—costing approximately $100 per day compared to 800 for hospital−based care. Strategic initiatives such as“Social Prescribing“and“Naturally Occurring Retirement Communities“(NORCs) are being implemented to address the social determinants of health, showing a high return on investment (4.43 for every $1 spent) and substantial reductions in emergency department visits (24%). This document synthesizes the current demographic reality, the challenges of senior poverty, and the proposed structural reforms for 2025 and beyond.
--------------------------------------------------------------------------------
1. The Demographic Reality: A Super-Aged Nation
In 2026, Canada surpassed a critical demographic threshold. The transition to an older society is not a sudden “tsunami” but a predictable shift that requires long-term planning beyond political cycles.
Current Statistics: 19% to 20% of the Canadian population is now aged 65 or older.
Projections for 2031: As the baby boom generation turns 85, one in four Canadians will be 65 or older.
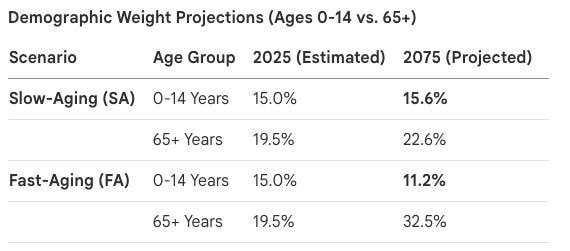
Long-term National Growth: Population projections suggest the national population could reach between 44 million and 75.8 million by 2075, with migration remaining the primary driver of growth.
Aging Acceleration: The number of individuals aged 85 and older is expected to triple by 2046, reaching approximately 2.5 million people.
--------------------------------------------------------------------------------
2. Senior Poverty and the Erosion of Dignity
Despite Canada’s status as a wealthy nation, a significant portion of the elderly population lives in precarious financial conditions. The “low-income measure” fails to capture the lived reality of many who are “getting better at doing without.”
Key Financial Challenges
The Poverty Line: 1 in 5 seniors live at the poverty line. Many rely on a “cobbled together” income of CPP and Old Age Security totaling roughly $2,000 a month, which is often entirely consumed by rent and inflation.
Hidden Poverty: Cases are documented of seniors living without heat or electricity in rural areas, or using “limiters” on their power to avoid total shut-offs.
Lack of Savings: Approximately 20% of older Canadians retire with only $5,000 in savings, and many still carry mortgages into retirement.
The “Fun” Gap: Seniors report a total lack of discretionary income after paying for necessities, leading to social isolation and depression.
Vulnerable Groups

3. Healthcare Evolution: Institutional vs. Community Care
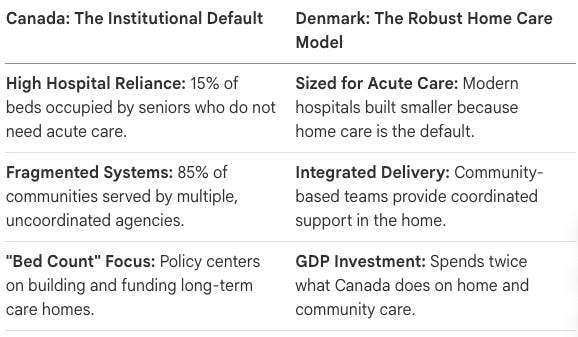
The current health system is described as being built for a 1965 demographic (average age 27). Experts argue that the system must catch up to the current reality where 15% of hospital beds are occupied by seniors who do not need acute care but have nowhere else to go.
Cost Analysis of Care Settings (Per Day)

Trends in Long-Term Care (LTC)
Ontario’s Ministry of Long-Term Care has outlined a four-pillar plan for 2025-2026:
Building Infrastructure: A commitment to 58,000 new or upgraded beds by 2028.
Service Funding: Expanding diagnostic testing (phlebotomy, ultrasounds) directly within LTC homes to reduce ER visits.
Staffing Supply: Increasing direct care to 4 hours per resident per day.
Accountability: Transitioning to the InterRAI reporting system by April 2026 for standardized assessments.
--------------------------------------------------------------------------------
4. Innovative Models: Vertical Cities and NORCs
With 37% of Toronto’s older adults already living in apartment buildings of five storeys or more (projected to reach 42% by 2041), the “Vertical City” model offers a high-density opportunity for efficient service delivery.
Naturally Occurring Retirement Communities (NORCs): These are buildings not originally designed for seniors but where a large number of residents have aged in place.
Place-Based Service Recommendations:
Priority Maintenance: Targeted snow clearance and cooling centers near high-density senior towers.
Mobile Programming: Bringing fitness classes and library services directly into building common rooms.
Transit Proximity: Reducing the “walkable distance” to bus stops from 300-1200m to 100-200m for NORCs.
Community Paramedicine: Utilizing paramedics for non-emergency diagnostic clinics within apartment buildings.
--------------------------------------------------------------------------------
5. Social Prescribing: Bridging Medical and Social Needs
Social prescribing is a formal referral pathway where healthcare providers direct patients to non-clinical, community-based supports (e.g., exercise groups, bereavement support, food security programs).
Impact and ROI
Economic Benefit: For every $1 invested, there is an estimated return of $4.43.
Utilization Reduction: Up to 24% reduction in emergency department visits and a 42% reduction in primary care appointments.
Person-Centered Care: Shifts the focus from “What is the matter with you?” to “What matters to you?”
Regional Highlights (2025)
Ontario: The Black-Focused Social Prescribing project addresses food insecurity and systemic barriers through Afrocentric care.
British Columbia: Over 100 community connectors are active as of April 2025, primarily through the “Better at Home” program.
Newfoundland & Labrador: Social navigators are being embedded into Family Care Teams to reach remote rural populations.
Quebec: The “Clic Social” platform streamlines referrals between clinicians and community organizations.
--------------------------------------------------------------------------------
6. Emerging Policy Directions
The document identifies several strategic directions for the 2023-2028 period:
Charter Challenges: Ongoing legal challenges against the federal government to force adequate funding of home care and palliative services, arguing that a lack of choice in care settings is a violation of dignity.
National Standards: Implementation of new national LTC standards (e.g., 4 hours of care) to be used by 72% of Canadian homes.
Integrated Care: Moving away from fragmented home care (where multiple agencies serve one building) toward a single responsible agency model to improve efficiency and worker stability.
AI Frameworks: Developing guidelines for AI use in health monitoring and decision-making for older adults to ensure equity and privacy.
Quiz & Answer Key
Instructions: Answer the following questions in 2–3 sentences based on the provided source context.
How is a “super-aged nation” defined according to the 2026 Canadian demographic context?
What is the estimated economic return for every dollar invested in social prescribing programs in Canada?
According to the NORC Innovation Centre, what percentage of older adults in Toronto are expected to live in “vertical communities” by 2041?
What are the “four pillars” of the Ontario Ministry of Long-Term Care’s plan to protect the healthcare system?
What specific financial and physical barriers did “Mary” from rural Alberta face while attempting to age at home?
What is the primary difference in hospital infrastructure between Canada and Denmark as described by Dr. Samir Sinha?
How does “social prescribing” function as a formal referral pathway?
What are the legislative targets for direct care hours in Ontario long-term care homes?
Why does Dr. Samir Sinha challenge the use of the term “tsunami” to describe the aging population?
What is the significance of “Afrocentric values” in the Black-Focused Social Prescribing project?
--------------------------------------------------------------------------------
Answer Key
Definition of a Super-Aged Nation: A nation is considered “super-aged” when at least 20% of its population (1 in 5 people) is aged 65 or older. Canada officially reached this demographic milestone in 2026.
Economic Return of Social Prescribing: Research indicates that every dollar invested in social prescribing programs in Canada yields an estimated return of $4.43. These programs contribute to a 24% reduction in emergency department visits and a 42% reduction in primary care appointments.
Seniors in Vertical Communities: By the year 2041, it is estimated that 42% of older adults in Toronto—approximately 285,000 people—will reside in “vertical communities” (buildings at least five storeys tall). This shift necessitates municipal policy changes regarding service delivery, such as localized snow clearance and transit accessibility.
The Four Pillars of Ontario’s LTC Plan: The plan is built on creating conditions to build new homes, funding system services and operations in both long-term care and the community, increasing the staffing supply to support direct resident care, and improving accountability through enforcement and transparency.
Barriers to Aging at Home (Mary’s Case): Mary lived at the poverty line, struggling with a $2,000-a-month income that left her unable to pay for both food and utilities. She faced “hidden poverty,” evidenced by the installation of a power limiter on her home that prevented her from using an oven or multiple appliances simultaneously.
Canada vs. Denmark Infrastructure: Denmark spends twice the percentage of its GDP on long-term care compared to Canada, focusing on robust home and community care. Consequently, Danish hospitals are built at a fraction of the size of current Canadian facilities because more citizens are supported in their own homes rather than occupying acute-care beds.
Social Prescribing Referral Pathway: Social prescribing allows healthcare providers to refer patients to non-clinical, community-based supports (such as exercise classes or social groups) to address social determinants of health. This process is facilitated by a “link worker” or “connector” who helps the individual navigate these resources.
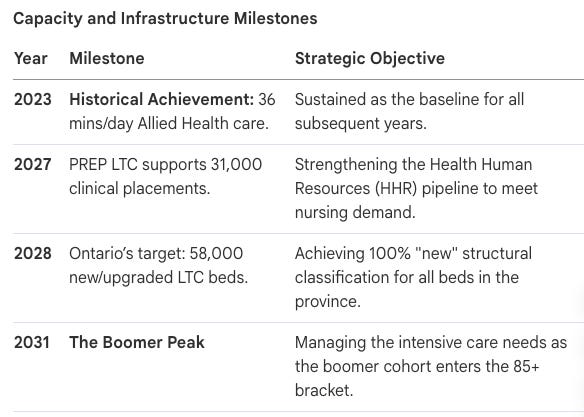
Ontario Direct Care Targets: The Fixing Long-Term Care Act, 2021 set a system-level target of 4 hours of direct care per resident per day from nurses and personal support workers by March 31, 2025. Additionally, the target for allied health professionals is set at 36 minutes of direct care per resident per day.
The “Tsunami” Concept: Dr. Sinha argues that “tsunami” implies a surprise event without warning, whereas the aging of the baby boomer generation has been a predictable demographic reality for decades. He suggests that the current crisis stems from a lack of advance planning by politicians who operate on short-term four-year election cycles.
Afrocentric Values in Social Prescribing: The Black-Focused Social Prescribing project uses Afrocentric principles to address systemic anti-Black racism and rebuild trust between health systems and Black communities. The model prioritizes culturally affirming care, food security, and Black representation in leadership and service provider roles.
Essay Questions for Further Reflection
Note: Answers are not provided for this section.
Economic Disparity in Aging: Analyze the concept of “hidden poverty” among Canadian seniors. How do rising housing costs, inflation, and the lack of workplace pensions create a scenario where seniors appear financially stable according to government measures but are unable to afford basic necessities?
The Vertical City Challenge: Evaluate the recommendations for the City of Toronto’s Third Seniors’ Strategy. How can urban planning, specifically regarding transit furniture and bus stop proximity, significantly impact the physical and mental well-being of seniors living in high-density apartment towers?
Institutionalization vs. Aging in Place: Compare the costs and outcomes of hospital-based care (800/day),long−termcarehomes(200/day), and home-based care ($100/day). Discuss the systemic barriers that prevent Canada from shifting toward the more cost-effective home-care model.
The Role of Social Prescribing in Preventive Healthcare: Discuss how social prescribing addresses the “social determinants of health.” Use examples from the provincial updates (such as British Columbia’s “Better at Home” or Ontario’s “Rx: Community”) to explain how non-medical interventions can reduce the burden on the acute healthcare system.
Demographic Projections and National Strategy: Statistics Canada projects a national population of up to 75.8 million by 2075, driven primarily by migratory increase. Discuss how these projections, combined with the “super-aged” status of the population, necessitate a shift from the 1965 “Medicare” model to a modern, integrated care system.
Glossary of Key Terms
Afrocentric Social Prescribing
A social prescribing model grounded in Afrocentric values to address systemic barriers and provide culturally affirming care for Black communities.
Ageism
Societal discrimination or prejudice against individuals based on their age, often leading to underfunded services for older adults.
Allied Health Professional (AHP)
Healthcare providers such as physiotherapists, occupational therapists, and social workers who provide specialized resident support.
Behavioural Supports Ontario (BSO)
A provincial initiative providing strategies and specialized staff to manage responsive behaviours associated with dementia or mental health issues.
Community Paramedicine
A program utilizing paramedics to provide non-emergency care, such as diagnostics and health monitoring, directly in a patient’s home.
Construction Funding Subsidy (CFS)
A financial incentive provided by the government to support the building or redevelopment of long-term care beds.
Link Worker / Connector
A dedicated professional who helps individuals navigate and access community-based services as part of a social prescription.
Naturally Occurring Retirement Community (NORC)
A building or neighbourhood not originally designed for seniors but where a high proportion of residents are aged 65 and older.
Social Determinants of Health (SDOH)
Non-medical factors, such as income, housing, and social connections, that account for more than 80% of a person’s health outcomes.
Social Prescribing
A formal referral pathway that connects patients from primary healthcare to community-based, non-clinical supports.
Super-Aged Nation
A demographic status reached when 20% or more of a country’s population is age 65 or older.
Vertical Community
High-density housing, such as apartment buildings or condominiums, that are at least five storeys tall.
Cast of Characters
1. The Demographic Backdrop: Setting the Stage for 2026
The year 2026 marks a definitive structural threshold for Canada. It is the year our nation officially reached “super-aged” status, a classification defined by Dr. Samir Sinha and international experts as the point where 20% of the population—one in five citizens—is aged 65 or older. While political rhetoric often frames this shift as a sudden “tsunami,” such language is strategically flawed. A tsunami implies an unpredictable catastrophe; however, the aging of the baby-boom generation has been a statistically visible reality for decades. This is a predictable demographic evolution that demands an immediate, structural departure from reactive policy-making toward long-term social infrastructure.
The following table illustrates the “Velocity of Aging” across various growth scenarios, highlighting the critical juncture of 2031, when the oldest baby boomers turn 85 and the demographic weight of seniors intensifies.
The Velocity of Aging: National Population Projections

The Strategic “So What?” These projections invalidate the current Canadian governance model, which remains trapped in a four-year political cycle. As Dr. Sinha notes, the number-one job of a health minister is often “to get re-elected” rather than to steward a long-term system. This misalignment necessitates a federal mandate for long-term planning, potentially adopting the Australian model of a unified national long-term care system. Without decoupling demographic stewardship from electoral volatility, Canada will remain perpetually “unprepared” for a future that is already here.
To understand the urgency, we must move from broad demographic projections to the individuals living within these numbers.
2. The Primary Protagonists: Seniors Navigating “Aging Without Dignity”
At the center of this transition are the seniors whose lived experiences reveal the systemic failure to provide “aging in place” with actual security. While 91% of seniors desire to stay in their own homes, a staggering one in five lives at the poverty line. We must reframe healthcare reform to address “hidden poverty,” where the choice between heat, food, and medication becomes the primary driver of health outcomes.
Case Personas: The Faces of Senior Poverty
The Rural Survivor (Mary): A 74-year-old in Alberta living on a $2,000 monthly income. Mary practices a form of “survivalist minimalism,” operating on an electricity “limiter” that cuts her power if she uses a toaster and oven simultaneously. She has endured periods without natural gas or hot water, treating “doing without” as a necessary adaptation to systemic neglect.
The Financial Regretter (Paul): A 77-year-old who finds himself in a “kill zone” where rising rent and food costs consume his entire pension. Paul represents the failure of private and public savings to withstand inflation, leaving him with no money for social engagement—what he terms a “huge mistake” in relying on the traditional retirement promise.
The Small-Town Invisible (Anne): A 62-year-old with chronic spinal pain whose struggle is compounded by the “psychological toll of visibility.” In a small community where she is known, the shame of relying on food banks leads to depression and social withdrawal. Her narrative highlights how poverty is not just a lack of funds, but a slow erosion of dignity and mental health.
The Strategic “So What?” Income inadequacy is a primary driver of “inappropriate” healthcare utilization. When Mary cannot afford air conditioning during a heatwave or Anne cannot afford nutritious food, they inevitably default to emergency departments. This transforms hospitals into expensive, inefficient social safety nets for social policy failures, treating symptoms of poverty with acute care resources.
The victims of this failure are now being championed by experts attempting to redesign the system from the ground up.
3. The Strategic Visionaries: The Geriatricians and Researchers
To move Canada beyond the “C grade” Dr. Sinha assigns its delivery of dignity, academic and clinical leaders are reframing aging from a medical burden into a social opportunity. Organizations like the National Institute on Ageing (NIA) and the CIHR Institute of Aging are advocating for a “home-first” philosophy that treats institutionalization as a last resort rather than a default.
The Economic Staircase: Denmark vs. Canada Canada remains an average spender that over-invests in institutional “warehousing” compared to Nordic models that prioritize home-based independence.
The Strategic “So What?” The economic logic of this transition is stark. As Dr. Sinha demonstrates, a day in a hospital costs 800∗∗,adayinalong−termcarebedcosts∗∗200, while a day of home care costs only $100. Realigning policy toward the $100-a-day model is the only fiscally sustainable path for a super-aged nation. Rejecting the term “tsunami” is essential for this shift; it moves the narrative from a disaster to be managed to a system to be designed.
This design must be applied specifically to where seniors increasingly live: our urban centers.
4. The Urban Architects: NORC Innovators and Vertical City Planners
In high-density “Vertical Cities” like Toronto, apartment towers are becoming Naturally Occurring Retirement Communities (NORCs). By 2041, an estimated 42% of Toronto’s seniors will live in these buildings. Researchers from the NORC Innovation Centre and Toronto Metropolitan University argue that these towers are the ideal settings for place-based service delivery.
“Design for Dignity” Recommendations:
Natural Densities: Leveraging vertical clusters to deliver on-site services (e.g., mobile vaccine clinics and fitness) directly to the lobby, reaching hundreds of seniors without requiring transit.
Urban Planning Reforms: Mandating 36-inch door widths and transit standards that place stops within 100-200m of senior-dense buildings. These specific standards prevent the “confinement” and “immobility” described by seniors who currently face 300-1200m walks to transit.
Climate Resilience: Establishing mandatory “Cool Spaces” within towers. This is a life-saving necessity; data shows that seniors in Toronto and Montreal experience significantly higher mortality rates from respiratory causes during extreme heat events.
The Strategic “So What?” “Vertical Aging” transforms isolated apartment units into “thriving vertical communities.” By building health and social infrastructure directly into the residential environment, we create a barrier against institutionalization and reduce the pressure on the long-term care waitlist.
The success of these vertical communities depends on the “connectors” who link residents to these services.
5. The Frontline Navigators: Social Prescribers and Link Workers
“Social Prescribing” acts as the formal bridge between clinical healthcare and community-based support, acknowledging that 80% of health outcomes are determined by social factors like housing and connection.
The Role of the Link Worker The system relies on Link Workers—non-clinical staff who co-create social prescriptions with patients—and Wellness Navigators who act as SDOH (Social Determinants of Health) experts. They translate a physician’s identification of loneliness or food insecurity into a tangible community connection.
According to the “Social Prescribing in Canada” report, the economic and clinical returns are undeniable:
Economic Return: $4.43 for every dollar invested.
System Relief: 24% reduction in emergency department visits.
Primary Care: 42% reduction in the need for primary care appointments.
The Strategic “So What?” This model shifts the medical paradigm from “What is the matter with you?” to “What matters to you?” It empowers seniors to lead their own health journey rather than being passive recipients of a fragmented system.
This grassroots innovation must now be balanced with the bureaucratic frameworks of the “Guardians.”
6. The Institutional Guardians: Ministries and Data Holdings
The Ontario Ministry of Long-Term Care and the Canadian Institute for Health Information (CIHI) manage the legislative and data-driven landscape of aging. Their focus is on accountability, bed capacity, and standardized reporting.
The Four Pillars of the Ontario 2025-2026 Plan:
Building Homes: A goal to open 30,000 net new beds and redevelop 28,000 existing beds by 2028.
System Funding: Targeted investments through the Local Priorities Fund to prevent unnecessary ER visits.
Staffing Supply: Achieving a target of 4 hours of direct care per resident per day by March 2025.
Accountability: Mandatory transition of all homes to the InterRAI reporting system by April 2026 to ensure standardized data across the system.
The Strategic “So What?” A strategic tension remains: the government continues to prioritize “bed counts” and institutional infrastructure while experts and seniors advocate for “home-first” models. While the Ministry is hitting its KPI for allied health care minutes, the system still struggles with a median wait-time increase for LTC placement. The challenge for these guardians is to move beyond managing a “warehouse” model and toward the community-integrated care of the future.
This future is being shaped by a new generation of equity-focused innovators.
7. The Future Guard: Students and Pharmacy Innovators
The final “characters” in this transition are moving from institutional management to equity-focused innovation. The Canadian Social Prescribing Student Collective (CSPSC) and the pharmacy sector are diversifying the aging workforce and addressing long-ignored health inequities.
Innovation Highlights:
Black-Focused Social Prescribing: This project addresses systemic anti-Black racism by grounding care in Afrocentric values. It recognizes that Black communities face disproportionate food insecurity (80% in some surveys) and requires culturally affirming programs to rebuild trust in the health system.
Pharmacy Integration: Pharmacists are emerging as accessible health hubs. In provinces like Ontario, they now screen for social determinants during routine consultations, acting as early-intervention navigators for social prescriptions.
Conclusion Canada’s transition to a super-aged nation is not a crisis to be feared, but a structural reality to be managed with foresight. Moving from a “C grade” in dignity to a world leader requires the seamless collaboration of all characters: the seniors like Mary and Anne sharing their survival truths, the researchers providing the $100-a-day evidence, the urban architects redesigning our towers, and the link workers bridging the gaps. By centering policy on human-centric narratives and long-term federal stewardship, Canada can ensure that 2026 marks the beginning of an era defined by dignity, choice, and connection.
Chronology of a Super-Aged Nation: Canada’s Healthcare and Demographic Evolution (2021–2075)
1. Strategic Context: The Proactive Shift in Canadian Gerontology
Tracking Canada’s transition into a “super-aged” nation—defined as the point where 20% of the population is aged 65 or older—is a strategic imperative that transcends mere data collection. It represents a fundamental reordering of the Canadian social contract. For policymakers, this timeline is not a countdown to a crisis but an existential imperative to transition the system from a reactive, hospital-centric “sick-care” model to a proactive, “wellness-infrastructure” model.
The “So What?” of this transition is rooted in systemic survival. The pivot from acute-care dominance to integrated community support, such as social prescribing and Naturally Occurring Retirement Community (NORC) based care, is the only viable strategy to prevent the bankruptcy of the healthcare system. By moving care “upstream” and leveraging social determinants of health (SDOH), the state can mitigate the burden on institutional settings. The groundwork for this transformation was laid in the early 2020s through a series of legislative and programmatic reforms.
--------------------------------------------------------------------------------
2. Foundations of Reform (2021–2024): Legislative and Programmatic Groundwork
Between 2021 and 2024, Canada established the regulatory and pilot-tested framework necessary to handle an aging population. Key initiatives shifted long-term care (LTC) and social care standards from the periphery to the center of the policy agenda.
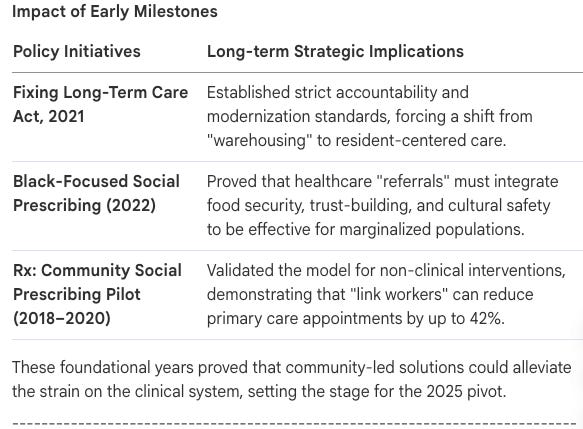
2021: Fixing Long-Term Care Act (Ontario): This landmark legislation committed $6.4 billion to build 58,000 new or upgraded beds by 2028. Critically, it mandated a system-level average of four hours of direct care per resident per day.
2022: Launch of Black-Focused Social Prescribing (BFSP) Project: This three-year initiative, implemented across four Black-led Community Health Centres, utilized Afrocentric values to address systemic barriers and anti-Black racism, providing culturally affirming care to improve health outcomes for racialized seniors.
2024: Conclusion of the 2020 LTC Staffing Plan: Ontario reported achieving 93% of its nursing and personal support worker (PSW) targets, adding over an hour of total daily direct care per resident since 2020.
3. The Pivot Point (2025): Trends and Vertical Innovations
By 2025, the strategic focus shifted toward “Vertical Innovation”—the practice of leveraging the natural density of urban living to deliver services more efficiently.
“8 Trends That Transformed Canadian Healthcare” Report: This report identified “Mobile Diagnostics” (such as phlebotomy and point-of-care testing) and “Place-Based Care” as the drivers of system modernization.
Aging in a Vertical City (June 2025): Published as part of Toronto’s Third Seniors’ Strategy, this report estimated that by 2041, 42% of older adults in Toronto will live in “vertical communities” (buildings 5+ storeys tall).
NIA Survey on Aging Optimism (June 2025): Documented a 5-point drop in optimism year-over-year, as seniors expressed increasing concern over economic instability and income adequacy.
Scaling the Social Prescribing Network: United Way British Columbia’s network of community connectors reached a critical mass of over 100 by April 2025, signaling the institutionalization of non-clinical referral pathways.
The Significance of Vertical Communities (NORCs)
Naturally Occurring Retirement Communities (NORCs) are buildings where a high proportion of residents are seniors. The system must capitalize on this natural density. In a NORC, a single community paramedic or social connector can serve dozens of clients in one building, eliminating the travel time that makes traditional home care inefficient. By using NORCs as hubs for mobile clinics and social programming, the system achieves the “place-based” efficiency required for a super-aged population.
--------------------------------------------------------------------------------
4. The Super-Aged Threshold (2026): A Year of Statistical and Human Crisis
In 2026, Canada officially became a super-aged nation, with 1 in 5 citizens (20%) aged 65 or older. This year saw a rapid acceleration of policy reports and the exposure of a growing human crisis.
January 20: NIA releases the 2025 Ageing in Canada Survey, revealing deep concerns regarding the high cost of aging and financial preparedness.
January 27: Statistics Canada releases population projections confirming the irreversible nature of Canada’s demographic shift.
February 17: CIHI releases the “Aging Without Dignity” podcast, and the NIA launches the Cost of Ageing (COA) Calculator to provide transparency on the true expense of later-life care.
March 5: NIA report: Understanding and Communicating the Value of Workplace Retirement Plans.
March 18: NIA report: Code of Conduct for the Prevention of Economic Abuse.
April 17: NIA Government Submission: Study on the Abuse and Financial Vulnerability of Senior Women.
April 21: NIA report: Developing an Artificial Intelligence Framework for the Health and Wellbeing of Older Canadians.
The Narrative of “Hidden Poverty”
The 2026 data shattered the “wealthy nation” narrative, revealing that 1 in 5 seniors live at the poverty line, with 20% retiring with less than $5,000 in savings.
“I went with no electricity and no natural gas... I’m just getting better at doing without.” — Mary, 74, Rural Alberta
“I have no money after I pay my rent to have fun. And I miss that.” — Paul, 77
“You don’t really like to show your face because it’s embarrassing... having difficulty in paying your bills or eating.” — Anne, 62, Rural North Toronto
This “hidden poverty” creates a cycle of systemic failure: food-insecure or isolated seniors end up in emergency departments, occupying beds at a much higher cost than would be required for community-based support.
--------------------------------------------------------------------------------
5. Mid-Term Targets and System Modernization (2027–2031)
Strategic planning for 2027–2031 focuses on the “Boomer Peak”—the year 2031, when the first baby boomers turn 85 and 1 in 4 Canadians will be 65 or older.
The Financial Mandate of Home Care
The shift to a home-care-first model is not a matter of preference; it is a financial mandate. The cost hierarchy is stark:
Hospital Bed: $800/day
Long-Term Care Bed: $200/day
Home Care Support: $100/day
To avoid system bankruptcy as the 85+ population explodes, the government must redirect funding toward the $100/day model.
--------------------------------------------------------------------------------
6. Long-Range Projections and Future Landscapes (2041–2075)
Demographic futuring allows policymakers to “future-proof” society for a landscape where the average age may reach 50.5 years.
2041: Estimates indicate 42% of Toronto seniors (285,000 people) will reside in vertical communities.
2046: The population aged 85+ will reach 2.5 million, a 3x increase from 2025.
2051: In Ontario, the senior population will grow from 18% (2023) to over 21%, representing 1.8 million new seniors.
Provincial Shifts (2050): The demographic weight of Quebec and Newfoundland and Labrador will decline. Alberta’s weight will increase, surpassing British Columbia in all scenarios except medium growth scenario M5.
2075: National population estimates range from 44M to 75.8M. Under “Fast-Aging” scenarios, 32.5% of the population will be seniors.
The Competitive Landscape of Caregiving
Dr. Samir Sinha warns of a projected 30% decrease in available family caregivers by 2050 due to smaller family sizes and geographic dispersion. In a society where family support is thinning, the state must fill the gap through standardized social prescribing and home care models.
Final Directive for Policymakers: The evolution from 2021 to 2075 dictates that Canada’s survival as a super-aged nation is predicated on the successful scaling of Social Prescribing and Vertical Community care. We must move from “warehousing” to “integrated living.” Failure to do so will result in a healthcare system that is not only financially insolvent but humanly unsustainable.
FAQ
Navigating Canada’s Transformation into a Super-Aged Nation
1. The Demographic Shift: Defining the “Super-Aged” Era
The year 2026 represents a permanent structural milestone in Canadian history. Demographic data from Statistics Canada and the Canadian Institute for Health Information (CIHI) confirm that Canada has officially crossed the threshold into a “super-aged” society. This transition is not an unforeseen “tsunami” but a predictable “slow-motion wave” resulting from decades of declining fertility and increasing longevity. Strategically, this shift requires a total reimagining of health infrastructure and urban planning, moving away from a system designed for a younger population toward one built for a reality where 1 in 5 citizens is a senior.
FAQ Synthesis
What are the official thresholds for a “super-aged” nation? A nation is designated as “super-aged” when 20% or more of its total population is aged 65 or older.
How do projections for the 85+ cohort through 2050 impact future health infrastructure requirements? The number of Canadians aged 85 and older—the cohort with the highest health and social care needs—is projected to triple by 2050, reaching approximately 2.5 million people. This “3x growth” represents a massive strain on current models of care, necessitating a shift from institutionalized beds to robust community-based support systems.
The “So What?” Layer The primary obstacle to effective management of this shift is “four-year cycle” political thinking. Governance typically prioritizes immediate outcomes for voters, which fundamentally conflicts with the long-term demographic realities of 2031 and beyond. By 2031, the first baby boomers turn 85; without 20-year planning horizons that look beyond the next election, the healthcare system will remain trapped in a reactive, expensive state of crisis.
--------------------------------------------------------------------------------
2. The Crisis of Economic Adequacy and “Hidden Poverty”
Income adequacy is a foundational social determinant of health that dictates healthcare system utilization. There is a dangerous gap between the public perception of senior wealth and the statistical reality of 2026, where “hidden poverty” is rampant. When seniors cannot afford basic necessities like nutrition or utilities, their health inevitably declines, leading to higher utilization of emergency departments—the most expensive sector of our health system.
FAQ Synthesis
Why are 1 in 5 Canadian seniors currently living at or below the poverty line? The “three-legged stool” of retirement—OAS/CPP, workplace pensions, and personal savings—has collapsed for many. Inflation in food and housing has outpaced fixed income, and a significant portion of the workforce lacks workplace pensions.
What are the primary drivers of “hidden poverty”? Key drivers include skyrocketing housing costs, the exhaustion of liquid savings, and the absence of indexed personal savings. Many seniors “cobble together” roughly $2,000 a month, which technically places them at the poverty line but leaves no margin for health-related costs.
Daily Barriers to Dignity: Qualitative Insights
Utility Rationing: Seniors using power limiters to avoid total disconnection, unable to use basic appliances like a toaster and microwave simultaneously.
Food Insecurity: Relying on food banks but experiencing deep “embarrassment” and loss of dignity in small communities.
Thermal Risk: Living without natural gas for hot water or air conditioning, the latter of which is now a lifesaving tool due to climate change.
Social Withdrawal: Having “no money left to have fun” after paying rent, leading to profound isolation and clinical depression.
The “So What?” Layer Systemic vulnerability is exposed by the fact that 20% of seniors enter retirement with only $5,000 in savings. A critical policy failure is the taxation of retirement income for those at the poverty line. As noted by seniors like “Anne,” taxing meager pensions when individuals are already struggling to eat is a systemic injustice. For the state, the cost of supporting a senior’s income is significantly lower than the $800-per-day cost of a hospital bed when that senior’s health fails due to poverty-induced neglect.
--------------------------------------------------------------------------------
3. Reimagining the Model of Care: Aging in Place vs. Institutionalization
While 91% of Canadian seniors desire to “age in place,” the current system remains heavily weighted toward institutional Long-Term Care (LTC). This misalignment is an economic failure; institutionalization is significantly more expensive than home care, and it frequently fails to provide the quality of life seniors expect.
FAQ Synthesis
What is the “math of care”? The daily cost discrepancy reveals the inefficiency of the current model:
Hospital Bed: ~$800/day
Long-Term Care Bed: ~$200/day
Home Care (LTC-eligible individual): ~$100/day
Why are 1 in 10 individuals entering LTC considered “potentially unnecessary” admissions? Data indicates that 10% of seniors are placed in institutional care simply because home and community supports—such as PSW visits or home modifications—were unavailable, not because their clinical needs actually required a bed.
The Four Pillars of Ontario’s Long-Term Care Strategy
Create Conditions to Build Homes: Focuses on increasing bed counts (target 58,000 new/upgraded beds by 2028). [Bed Capacity]
Fund System Services and Operations: Addresses diagnostic access, local priorities, and community paramedicine. [Aging in Place]
Increase Staffing Supply: Targets 4 hours of direct care through recruitment and training. [Bed Capacity / Retention]
Improve Accountability and Transparency: Implements the InterRAI system and proactive inspections. [System Integrity]
The “So What?” Layer Canada’s GDP spend on long-term care is anemic compared to Nordic benchmarks. Denmark spends nearly double the percentage of GDP on long-term care than Canada. Because Denmark invested heavily in the “Aging in Place” model, their hospitals are actually being built smaller—the direct result of successfully shifting care into the home. Until Canada matches this ROI-focused investment, emergency departments will remain overcrowded with “ALC” (Alternate Level of Care) patients.
--------------------------------------------------------------------------------
4. The Innovation Frontier: NORCs and Vertical Living
Naturally Occurring Retirement Communities (NORCs)—residential buildings where at least 30% of the population is 65+—represent a strategic opportunity to modernize service delivery. By leveraging “natural density” in high-rise environments, the health system can deliver care with unprecedented efficiency.
FAQ Synthesis
What defines a “Vertical NORC,” and why will 42% of Toronto seniors live in one by 2041? Vertical NORCs are multi-unit high-rises not originally built for seniors that have evolved to house high concentrations of older adults. In Toronto, the proportion of seniors in these settings is expected to rise from 37% to 42% by 2041.
How can municipal services be optimized for vertical communities? Shifting from “horizontal” delivery (visiting individual houses) to “vertical” delivery (on-site lobby clinics) allows a single provider to see ten times as many patients in the same timeframe.
Recommendations for Aging in a Vertical City
Prioritized Snow Removal: Treat the sidewalks around high-density senior buildings as “Safety Zones” to prevent falls and isolation during winter.
Mobile Fitness and Senior Classes: Repurpose building common rooms as satellite community centers, bringing Parks and Rec programs directly to frailer residents.
Transit Accessibility Standards: Reduce the “walk to bus stop” standard from 300m to 100m for stops near NORCs. Currently, 35% of bus stops near NORCs have no furniture; all must be equipped with shelters and benches to support mobility.
Community Paramedicine Clinics: Expand the “CPLC Plus” model where paramedics hold regular “drop-in” hours in lobbies to monitor chronic conditions and provide on-site diagnostics.
On-site Vaccine Clinics: Use the density of high-rises to run seasonal flu and COVID-19 clinics, significantly increasing uptake by removing transportation barriers.
The “So What?” Layer The transition from horizontal to vertical service models is not just about convenience; it is about the Return on Investment for public health. Density reduces the “barrier to entry” for frailer seniors. When a vaccine clinic is held in a lobby rather than across town, uptake increases among those most at risk, directly preventing the high-cost hospitalizations that follow a flu or COVID outbreak.
--------------------------------------------------------------------------------
5. Holistic Health: Social Prescribing and Mental Well-being
Social prescribing represents a transformative shift in healthcare, moving from the clinical inquiry of “What’s the matter with you?” to the person-centered inquiry of “What matters to you?” As social determinants (SDOH) account for 80% of health outcomes, clinical medicine alone is an incomplete solution.
FAQ Synthesis
What is the estimated Return on Investment (ROI) for social prescribing programs in Canada? For every $1.00 invested in social prescribing, there is a return of $4.43 in social and economic value.
How does a “Social Prescription” differ from a medical one, and who are “Community Connectors”? A social prescription is a formal referral to a non-clinical activity (e.g., arts, nature, or food security). Community Connectors (or Link Workers) act as the vital bridge, addressing the 80% of health outcomes driven by SDOH by solving root causes—like food insecurity or isolation—before they manifest as clinical crises.
Impact Areas and Case Studies
Culturally Affirming Care: Black-Focused Social Prescribing addresses systemic racism by connecting Black seniors to Afrocentric community and food security supports.
Arts and Mental Health: Opera Makers and Arts on Prescription initiatives reduce the “hermit-like” existence of isolated seniors through storytelling and music.
Pharmacy-led Initiatives: Leveraging community pharmacists as “trusted hubs” to screen for loneliness and provide social referrals alongside medication reviews.
Indigenous Nature Prescribing: Utilizing land-based healing and traditional knowledge to improve mental and spiritual well-being.
The “So What?” Layer Social prescribing is the key to “unburdening” the clinical workforce. Data confirms that these programs lead to a 24% reduction in ER visits and a 42% reduction in primary care appointments. By utilizing Link Workers to solve social root causes, physicians can focus their limited time on complex medical cases rather than acting as default social workers.
--------------------------------------------------------------------------------
6. Policy, Accountability, and the Path Forward
A national standard for aging with dignity is essential. Currently, access to quality home care is a “geographical lottery,” which is unsustainable in a super-aged nation.
FAQ Synthesis
What are the “Fixing Long-Term Care Act” targets for direct hours of care (DHOC)? The legislated target is 4 hours of direct nursing/PSW care per resident, per day. As of late 2024, Ontario had reached 93% of this goal.
How will the transition to the “InterRAI” reporting system by 2026 improve accountability? By April 2026, all LTC homes must adopt InterRAI, a standardized tool that tracks resident health quarterly. This allows for national benchmarking and data-driven policy adjustments.
KPI Checklist for the Super-Aged Healthcare System
[ ] National Standards Accreditation: Target 100% of LTC homes accredited under the new National LTC Standards (currently at 72%).
[ ] Bed Modernization: 100% of provincial LTC beds classified as “new” structural standards by 2028.
[ ] Proactive Compliance: 100% of LTC homes receiving annual proactive provincial inspections.
[ ] Wait Time Reduction: Achieving a downward trend in median wait times for home care and LTC placement.
[ ] Diagnostic Integration: Expansion of “CPLTC Plus” (Community Paramedicine) to all high-density senior settings.
The “So What?” Layer The ongoing “Charter Challenge” led by Dr. Samir Sinha highlights a critical ethical crisis: Canada provides Medically Assisted Dying (MAID) as a fully covered option, yet home care and LTC remain a constant struggle to access. This dichotomy frames the current system as a potential human rights violation. A society that provides an efficient path to death but an arduous path to dignified living is a society in failure. The path forward requires a system that treats home care as a right, ensuring that MAID is never a “choice of poverty.”
Note: Use of population data is governed by the Statistics Canada Open Licence Agreement. Projected data is based on Statistics Canada (2026) and CIHI (2026) reporting.
Table of Contents with Timestamps
Introduction — 00:00 The Heliox signature opening: independent, moderated, timely conversations about things that matter. Breathe easy — we go deep and lightly surface the big ideas.
The Two-Act Play We’re Living In — 00:25 The hosts frame human life as a cultural script with a missing third act. Childhood, adulthood — and then, largely, silence. A provocative opening premise about how we’ve misread the story of aging entirely.
Canada Crosses the Threshold — 01:11 A landmark demographic milestone: Canada is now officially a “super-aged” nation. One in five Canadians is over 65. Medical systems, social safety nets, and city infrastructure are facing a reality they were never built for — and had 40 years to see coming.
Introducing Dr. Louise Aronson and the Mission — 01:46 Meet today’s guiding expert: geriatrician Dr. Louise Aronson and her sweeping book Elderhood: Redefining Aging, Transforming Medicine, Reimagining Life. The episode’s triple mandate is declared: deconstruct the biology, the economics, and the architecture of aging.
The Word “Old” — How Language Shapes Value — 02:48 Dr. Mikko’s word association exercise reveals the depth of our cultural conditioning. The word “old” generates universally negative associations; “elder” flips the psychology entirely. The label, it turns out, literally dictates the perceived value of a human being.
The Napkin Graph and the Silver Tsunami — 04:15 A bleak sketch on a coffee shop napkin captures our monolithic view of aging as relentless decline. The hosts unpack the damaging metaphor of the “silver tsunami” and why framing demographic success as catastrophe is a profound psychological inversion.
Elderhood as a Distinct Life Stage — 06:36 Dr. Aronson’s proposed revised life cycle: childhood, adulthood, and elderhood — each spanning decades, each with its own distinct developmental phases. The physiological differences between a 65-year-old and a 95-year-old are as vast as between a newborn and a 30-year-old.
Othering and the Psychology of Avoidance — 07:54 Drawing on Simone de Beauvoir, the episode explores “othering” as a psychological defense mechanism — how we strip older adults of nuance to protect ourselves from the cognitive dissonance of our own mortality.
When Age-Blindness Becomes Dangerous Medicine — 09:01 Patient Anne Rowe, 89, nearly dies when standard adult medical protocols fail to account for the physiological realities of elderhood. The story catalyzes Dr. Aronson’s life’s work in geriatrics.
Mabel, Eva, and the Mechanic Shop Model — 11:01 Two ER case studies expose systemic age bias: a toxicology screen ordered for a bed-bound 94-year-old, and a patient in her 80s prescribed 17 medications by five specialists — none of whom asked about her daily life. Medicine optimizes organs while ignoring the person living inside them.
The Medicalization of Aging — 14:53 How aging was transformed from a natural life stage into a series of billable defects. The origins of a healthcare model that prioritizes acute intervention over functional independence.
A 2,000-Year-Old Debate: From Aristotle to Marjorie Warren — 15:54 The philosophical fault lines about aging trace back to ancient Greece. Aristotle’s fatalistic “pneuma” theory versus Cicero and Galen’s proto-geriatric advocacy. And then the transformative work of Dr. Marjorie Warren in 1930s Britain, who proved that so-called “hopeless” patients could regain functional independence with specialized care.
The Hidden Curriculum and the Billing Code Problem — 19:09 Why does geriatrics barely appear on hospital websites? The unspoken culture passed from attending physicians to residents, combined with billing codes designed for speed, structurally penalizes the slow, thorough work that keeps elders healthy.
The Economics of Elder Poverty — 20:58 CIHI data reveals one in five older Canadians lives below the poverty line. Through Mary, Paul, and Anne — three real individuals from the documentary Aging Without Dignity — the human cost of structural underfunding becomes impossible to look away from.
MAID, Autonomy, and the Charter Challenge — 25:03 A sober examination of how poverty and inadequate home care intersect with Canada’s Medical Assistance in Dying framework. A legal and ethical debate about whether a genuine choice exists when the alternatives are a freezing home, institutionalization, or assisted death.
The Political Life Cycle vs. the Human Life Cycle — 26:21 Why governments built for four-year election cycles cannot plan for forty-year demographic shifts. Australia’s federalized long-term care model as a counterexample of political will done right.
Healthspan Over Lifespan: The Geroscience Revolution — 27:44 The most radical reimagining of aging is biological. The shift from extending lifespan to extending healthspan — compressing the period of chronic disease so that vitality persists until very near the end of life.
Zombie Cells and the Biology of Inflammaging — 29:32 Cellular senescence explained: the Hayflick limit, telomere shortening, and the “zombie cells” that secrete the toxic SASP cocktail driving inflammation, arthritis, heart disease, and cancer. Senolytic therapies are being developed to hunt and clear these cells.
Redefining “Old” — The Mortality Risk Metric — 31:06 Stanford economist John Chauvin’s proposal: define old age not by chronological years but by statistical mortality risk. By this biological measure, the threshold for “old” has been pushed back nearly two decades since 1920 — yet our social systems remain anchored to a mid-twentieth century calendar.
Silver Architecture and Designing for Human Bodies — 32:56 From individual buildings to entire cities: how tactile flooring, acoustic dampening, high-contrast lighting, and accessible design transform impairments from debilitating handicaps into manageable differences.
NORCs: Distributed Care and the Danish Model — 34:43 Naturally Occurring Retirement Communities bring clinical care directly into the buildings where seniors already live. New Brunswick’s “Nursing Home Without Walls” program and Denmark’s national model demonstrate that community-based care simultaneously improves outcomes and dramatically reduces costs.
Dismantling “Successful Aging” — and Inez — 37:49 The toxic mythology of the “successful aging” framework, which defines thriving as mimicking a middle-aged body. Against this metric, the quiet humanity of Inez — bed-bound, cognitively impaired, still winking, still joking — offers a profound counter-argument. Joy and meaning do not evaporate when a body becomes frail.
The New Metric: Adaptation and Elderhood’s Distinct Value — 41:04 Anthropologist Margaret Clark’s research: elders who thrive are not those clinging to youth, but those who have consciously adapted — embracing community, self-acceptance, and wisdom over professional status and physical dominance. They succeeded at elderhood, not at remaining middle-aged.
Synthesis and Closing Philosophical Question — 41:57 The episode’s threads are woven together. A final, provocative question: if we succeed in redesigning society to honor elderhood as a rich developmental stage, will our evolutionary fear of death actually change — or will the human mind simply find a new frontier to fear?
Outro and Credits — 43:42 Closing invitation to question systems, demand better data, and see elders — and our own futures — with fresh eyes. Production credits, podcast philosophy, and four recurring narrative frameworks: boundary dissolution, adaptive complexity, embodied knowledge, and quantum-like uncertainty.
Index with Timestamps
Acute care hospitals, costs of, 24:04
Adaptation, psychological, in elderhood, 41:08, 41:23
Age-blindness in medicine, 07:40, 09:01, 12:51
Aging, medicalization of, 14:53
Aging, as natural developmental stage, 16:49, 37:55
Aging Without Dignity (CIHI documentary), 21:39
Aristotle, pneuma theory, 16:05
Aronson, Dr. Louise, 01:55
Australia, federalized elder care, 27:05
Autonomy, dignity and, 23:13, 25:28
Baby boomers, demographic tracking, 06:03
Billing codes, structural bias in, 20:12, 20:46
CIHI (Canadian Institute for Health Information), 02:22, 21:10
CIHR Institute of Aging, 02:31, 27:51
Cicero, advocacy for elderhood, 16:42
Clark, Margaret, anthropologist, 41:08
Cognitive dissonance, mortality and, 08:35
Delirium, as misdiagnosed condition, 11:52, 12:22
Denmark, elder care model, 36:42
Elder, word association exercise, 03:46
Elderhood, as distinct life stage, 06:55, 07:07
Elderhood (book by Dr. Aronson), 01:57
Eva, polypharmacy case study, 13:16
Frailty, as biological reality, 38:48, 39:11
Galen, proto-geriatric advocacy, 16:45
Geriatrics, coining of term, 17:20
Geriatrics, hidden curriculum, 19:26
Geroscience, 28:59, 29:03
Geroscience, CIHR strategic plan, 27:51
Hall, Donald, octogenarian poet, 08:22
Hayflick limit, cellular biology, 29:36
Healthspan vs. lifespan, 28:20
Hidden poverty, elder Canadians, 21:10
Home care, cost comparison, 24:28
Hospitalization costs, acute care vs. home care, 24:04
Impairment vs. handicap distinction, 33:23
Inflammaging, 30:29
Inez, patient narrative, 39:24
Institutionalization, economic drivers of, 23:39
John Chauvin, mortality risk metric, 31:25
Language and aging, cultural impact, 02:48, 03:37, 40:21
Lifespan vs. healthspan, 28:08
Long-term care, costs of, 24:16
MAID (Medical Assistance in Dying), 25:03
Mary, rural Alberta case study, 21:51
Medicare, designed 1965, 26:02
Mikko, Dr., word association exercise, 02:54, 04:15
Mabel, emergency room case study, 11:10
Napkin graph, downward trajectory, 04:24
Naturally Occurring Retirement Communities (NORCs), 34:43, 34:49
New Brunswick, Nursing Home Without Walls, 35:38
“Old,” word association exercise, 03:10, 03:30
Old, reclaiming the word, 40:21, 42:43
Othering, psychological mechanism, 07:54, 08:12
Paul, pension case study, 22:44
Pneuma, Aristotle’s life force theory, 16:11
Political life cycle, institutional myopia, 26:21
Polypharmacy, dangers in elderhood, 13:37
Poverty, hidden, among elders, 21:10
Roe and Kahn, 1997 successful aging study, 38:03
SASP (Senescence Associated Secretory Phenotype), 30:15
Senescence, cellular, 29:26, 30:04
Senolytic therapies, 30:47
Silver architecture, 33:04, 33:18
Silver tsunami, metaphor critiqued, 05:08, 05:37
Simone de Beauvoir, othering theory, 08:01
Sinha, Dr. Samir, geriatric specialist, 05:14, 20:10
Successful aging, toxic mythology of, 37:55, 38:15
Super-aged nation, Canada 2026, 01:20
Telomeres, shortening with age, 29:36
Warren, Dr. Marjorie, mother of British geriatrics, 17:45, 18:05
Wisdom, associated with “elder,” 03:55
Word association exercise (old vs. elder), 02:54, 03:46
Zombie cells, senescent cells, 30:04, 30:38
Poll
Post-Episode Fact Check
The following claims from the episode have been assessed for accuracy based on available published research, institutional data, and expert literature. Overall assessment: the episode is well-sourced, accurate, and appropriately qualified.
CLAIM: “Canada has officially crossed the demographic threshold — we are now a super-aged nation, with one in five people over the age of 65.” ASSESSMENT: Accurate and timely. A “super-aged society” is defined by the WHO and World Bank as one in which 20% or more of the population is aged 65+. Statistics Canada data and projections from CIHI have indicated Canada would cross this threshold around 2024–2026. The claim is well-supported.
CLAIM: “We had 40 years to prepare for this demographic shift.” ASSESSMENT: Accurate. Canada’s baby boom cohort (born approximately 1946–1964) reaching 65+ was a documented and projected demographic event for decades. Numerous federal and provincial planning documents have flagged this transition since at least the 1980s.
CLAIM: “The term ‘silver tsunami’ was coined in the 1980s.” ASSESSMENT: Broadly accurate. The phrase emerged in popular and policy discourse in the 1980s and gained significant traction through the 1990s and 2000s, particularly in American and Canadian healthcare policy circles. Its exact coinage date is disputed, but the 1980s attribution is defensible.
CLAIM: Dr. Louise Aronson is the author of Elderhood: Redefining Aging, Transforming Medicine, Reimagining Life. ASSESSMENT: Confirmed. Published by Bloomsbury in 2019. Dr. Aronson is a geriatrician at the University of California San Francisco. The book won several awards including the PROSE Award.
CLAIM: “The physiological differences between a healthy 65-year-old and a 95-year-old are as vast as the differences between a newborn and a 30-year-old.” ASSESSMENT: This is a reasonable qualitative analogy used in geriatric medicine education, not a precise quantitative claim. The underlying point — that flattening 30 years of physiological change under a single clinical category is medically unjustified — is well-supported in geriatric literature.
CLAIM: Treating older patients with middle-aged adult protocols can be dangerous due to decreased renal clearance and altered cytochrome P450 enzyme metabolism. ASSESSMENT: Accurate. These are well-established principles in clinical pharmacology and geriatrics. Age-related changes in renal function and hepatic metabolism extend drug half-lives and increase toxicity risk. This is documented extensively in pharmacogeriatrics literature.
CLAIM: “One in five older Canadians is living at or below the poverty line.” ASSESSMENT: This statistic requires some qualification. Elder poverty rates in Canada vary significantly by methodology and definition. Low Income Measure (LIM) data suggests approximately 11–15% of seniors live below the LIM threshold in recent years, though some subpopulations (women living alone, recent immigrants, Indigenous seniors) face much higher rates. The “one in five” figure may reflect broader definitions or more recent data trends. Listeners should consult the specific CIHI data source cited.
CLAIM: “It costs approximately $800 a day to maintain an older adult in an acute care hospital bed while waiting for placement, $200 a day in long-term care, and $100 a day for robust home care.” ASSESSMENT: These figures are broadly consistent with CIHI and provincial health ministry estimates for Canada, though specific numbers vary by province and year. The ratio (home care being significantly cheaper than institutional care) is consistently supported in the literature. These figures are appropriately approximate and directionally accurate.
CLAIM: MAID and elder poverty intersection — that a subset of older adults in poverty are exploring MAID.ASSESSMENT: This is a documented and actively debated policy reality in Canada. Multiple journalistic investigations, parliamentary testimony, and the Canadian Human Rights Commission have flagged cases in which individuals have cited lack of adequate social support as a driver of MAID requests. The claim is factual and the charter challenge referenced is a real legal proceeding.
CLAIM: “Medicare was designed in 1965 when the average Canadian was 27 and life expectancy was significantly lower.” ASSESSMENT: Canada’s national Medicare framework (the Medical Care Act) received royal assent in 1966 and took effect in 1967. The median age of Canadians in the mid-1960s was approximately 26–27. Life expectancy at birth in Canada in 1965 was approximately 72 years (vs. approximately 82+ today). The claim is accurate in spirit.
CLAIM: The Hayflick limit — cells can only divide a finite number of times — and telomere shortening as a mechanism of aging. ASSESSMENT: Confirmed. The Hayflick limit was described by Leonard Hayflick and Paul Moorhead in 1961. Telomere shortening as a driver of cellular senescence and aging is extensively documented. This is foundational biology.
CLAIM: Senolytic therapies are being developed to clear senescent “zombie cells” and delay age-related disease.ASSESSMENT: Accurate. Senolytic compounds (including dasatinib + quercetin, navitoclax, and others) are in active clinical trials as of 2025–2026 for conditions including osteoarthritis, cardiovascular disease, and frailty. The field of geroscience is real and rapidly evolving, though clinical applications in healthy aging contexts are still largely experimental.
CLAIM: “A woman in 1920 hit the 2% annual mortality risk threshold at age 55; today she does not reach it until age 73.” ASSESSMENT: This references the work of economist John Shoven (note: the transcript renders his name as “Chauvin,” which appears to be a phonetic approximation of “Shoven”). John Shoven of Stanford has published extensively on mortality-based definitions of old age. The specific ages cited are consistent with his published work and U.S./Canadian demographic mortality tables. The discrepancy in name spelling is worth noting.
CLAIM: Denmark is building hospitals significantly smaller than Canadian/American equivalents due to a shift to community-based elder care. ASSESSMENT: Broadly accurate. Denmark has invested heavily in home and community-based care for decades and has consequently reduced reliance on acute care hospital beds. Danish hospitals are generally smaller per capita than Canadian or American counterparts. The causal narrative presented is somewhat simplified but directionally supported.
CLAIM: The 1997 “successful aging” framework by Rowe and Kahn. ASSESSMENT: Accurate. John Rowe and Robert Kahn published “Successful Aging” in The Gerontologist in 1997, defining three components: low disease risk, high cognitive/physical functioning, and active engagement. The critique that this framework pathologizes natural decline is a documented and ongoing debate in gerontology.
CLAIM: Margaret Clark’s anthropological research on thriving in old age through adaptation. ASSESSMENT: Accurate. Margaret Clark conducted cross-cultural research on values in aging, finding that those who thrived tended to actively reorient their value systems away from productivity and dominance toward connection, acceptance, and wisdom. This work is cited in gerontological literature.
OVERALL FACT CHECK RATING: Strong. The episode demonstrates rigorous sourcing across multiple institutional and academic references. Minor cautions: the elder poverty statistic may warrant a footnote specifying the exact CIHI methodology; the name “Shoven” vs. “Chauvin” is worth correcting in show notes; and senolytic therapies should be framed as promising but still largely in clinical trial phases. No significant inaccuracies identified.
Image (3000 x 3000 pixels)

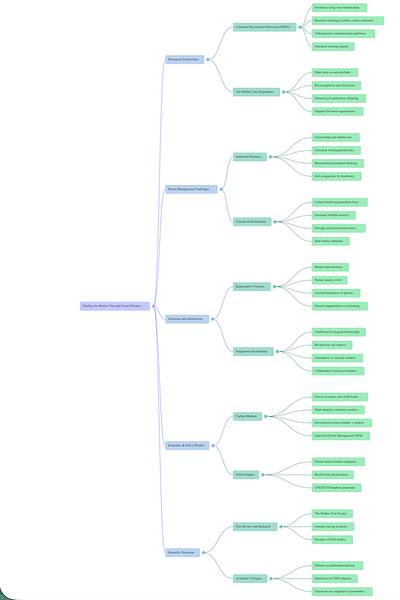
Mind Map
Comic
Street Art
Infographics